17 Upper lid blepharoplasty
INDICATIONS
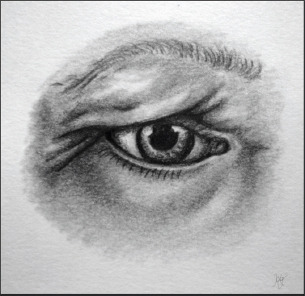
The indications for upper lid blepharoplasty are of both aesthetic and functional importance. Patients present with aesthetic concerns corresponding to findings on physical exam. Common symptomology includes periorbital wrinkles, redundant upper eyelid skin, low supratarsal fold, upper lateral periorbital rhytids, or peripheral visual field deficits (Figure 17.1).
Note: Certain medical conditions increase the risk of complications and should be evaluated prior to upper lid blepharoplasty. Included in these conditions are
Autoimmune disorders (collagen vascular diseases)
Grave disease
Eyelid inflammatory disorders
Benign essential blepharospasm
Dry eye syndrome
INTRODUCTION
The goals of upper lid blepharoplasty are to restore upper orbital shape and a defined upper lid crease. The procedure is intricate and challenging. With proper preoperative assessment and planning, one can have excellent aesthetic and functional outcomes.
Upper lid blepharoplasty requires careful preoperative assessment. A detailed history and physical that focuses on the orbit, brow, lid, and midface must be obtained. The patient should be sent for a formal ophthalmologic exam for evaluation and clearance.
Patients at risk for dry eye should be evaluated in the office as part of the preoperative assessment using the Schirmer test; this will help guide perioperative planning and postoperative care. Patients should also be assessed for ptosis, asymmetry, height of supratarsal fold, lagophthalmos, brow position, as well as lacrimal gland prolapse. This chapter focuses purely on the aesthetic procedure, but it should be noted that a functional procedure may be necessary based on the findings in the preoperative evaluation. Table 17.1 indicates special equipment needed.
PREOPERATIVE MARKINGS
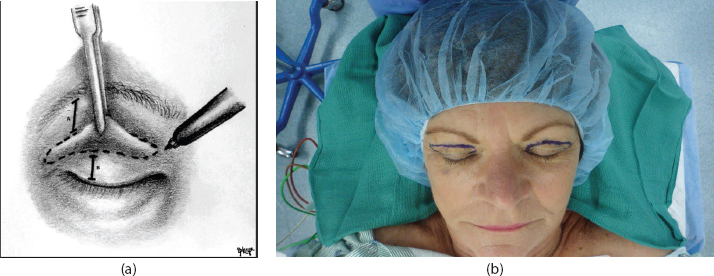
To obtain precise preoperative markings, the current preferred practice is to have the patient sitting in the preoperative area. The surgeon may obtain markings with the aid of loupe magnification and with caliper measurements to confirm symmetry of markings bilaterally (Figure 17.2).
Mark the upper eyelid crease at the level of the mid-pupillary line.
In women: ∼10 mm superior to the lash margin
In men: ∼8 mm superior to the lash margin
This marking should be tapered caudally at the nasal and lateral eyelid margins so that it follows the curve of the upper eyelid crease.
Do not extend the nasal aspect too far medially; this will avoid webbing or epicanthal folds above the medial canthus.
The amount of tissue to be excised nasally should be conservative because over-resection of skin and muscle can lead to poor aesthetic outcomes and result in lagophthalmos and corneal exposure and dryness.
The lateral marking should be ∼5–6 mm above the lash line. We mark the lateral extent of our incision at a point where the redundancy ends within a periorbital rhytid.
To determine the superior margin of the excision, pinch and identify the quantity of excess skin and muscle.
At minimum, 10 mm (some authors say 15 mm) of skin should be preserved between the lower border of the eyebrow and the upper eyelid marking at the level of the lateral canthus.
To complete the superior mark, follow a gentle curve that parallels the contour of the lower marking and taper nasally to reduce the amount of skin and muscle that is removed along the nasal half of the incision. We sometimes angle the last portion of the nasal aspect of the incision at a 45° angle upward (not shown).
Pay attention to the presence of eyebrow and eyelid fold asymmetry, because if asymmetrical brow positions are present preoperatively, the upper eyelid markings should closely approximate one another, but a concurrent procedure should be planned to correct brow position.
Symmetry can be achieved by removing different amounts of skin and muscle during the operative procedure.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


