17 Lateral Epicondylar Debridement
Abstract
This chapter on lateral epicondylar debridement will review some of the techniques available for surgical treatment of recalcitrant lateral epicondylitis (LE) and focus on the author’s preferred methods of treatment. There is general consensus in the literature that the vast majority of cases of lateral epicondylitis resolve within 6 to 12 months regardless of nonoperative treatment choices and that up to 10 per cent of cases will be treated with surgery. 1 The author’s preferences will be discussed with detailed description of nonoperative care and surgical technique as well as immediate postoperative care and rehabilitation. Potential complications will be discussed. The goal of this chapter is to provide the reader with an understanding of the available choices, and discuss a safe, reproducible, effective and commonsense methodology and (when needed) surgical technique for treating intractable tennis elbow.
17.1 Background
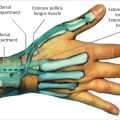
It could be said that a lack of consensus is a consistent finding when one reviews the literature on lateral epicondylitis (LE) and its treatments. LE stands as an example of a diagnosis where many surgeons are convinced that their treatment protocol gets the best results, but the irony is that no one best evidence-based treatment has ever surfaced. There are, however, some features of this condition that have been accepted since the classic article by Nirschl and Pettrone in 1979. There has been a general consensus that the tissue found at the site of the extensor carpi radialis brevis (ECRB) origin at the lateral epicondyle and supracondylar ridge of the distal humerus is angio-proliferative in nature, and the histopathologic findings have been termed angiofibroblastic hyperplasia. 2 The pathology can extend to the origins of extensor carpi radialis longus (ECRL), extensor digitorum communis (EDC), and even extensor carpi ulnaris (ECU). The pathology is not true “inflammation” as its suffix “-itis” would imply. LE preferentially affects the dominant extremity. It is also widely accepted that nonoperative treatment is the default approach for new onset “tennis elbow.”
17.2 Nonoperative Treatment
Nonoperative treatment methodology runs the gamut from patient counseling alone, activity modification, corticosteroid injections, counterforce bracing during the waking hours/cockup wrist splinting during sleep to formal therapy. Therapeutic techniques include frictional massage, iontophoresis, low-intensity ultrasound, stretching of the extensor muscles, and alternating heat and ice application. Some practitioners promote the use of high-intensity ultrasonic shock wave treatment for LE, but there remains skepticism about its effectiveness and high cost. The same concerns exist about plasma rich protein and autologous blood injections into the ECRB origin; these two modalities have not gained widespread appeal.
17.2.1 Author’s Preferred Method for Nonoperative Treatment
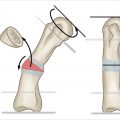
The author’s preferred methodology for nonoperative treatment of LE is dependent on patient examination and the chronicity of the condition upon presentation. If the patient presents with a chronic and untreated LE, especially if they present with a flexion contracture of the elbow, or if passive extension of the elbow provokes lateral elbow pain, then formal therapy is initiated first, combined with patient education, activity modification, a home exercise program, and use of counterforce brace (CFB). We have anecdotally found “clasp” devices are more effective at controlling the pain with activities of daily living (ADLs) than the traditional single-ply TES. This may be because the clasps and padded TESs more accurately focus the counter force pressure on the extensor muscle group. In addition, the effectiveness of CFBs is dependent upon their proper positioning. Often, patients present to the office with straps that they have positioned directly over the lateral epicondyle. We recommend applying the CFB three finger breadths below the extensor tendon origin, centered on the midline of the extensor muscle group. Patients are instructed to tension the device compression, so that when they make a fist, they feel ample and comfortable compression of the extensor muscles, but when relaxed there is no constriction of the forearm. For patients with more acute localized LE and no elbow contracture, we provide education, offer a corticosteroid injection, and direct the patient on a home exercise program. The goal is to let them recover, on their own, for as long as they can endure, because the probability is overwhelmingly in favor of recovery with self-care and without surgery.
17.3 Differential Diagnosis
Compression of the posterior interosseous nerve (PIN) at the arcade of Frohse at the distal end of the supinator, or radial tunnel syndrome (RTS), is reported to be present in approximately 5 percent of patients with LE. 3 Electromyogram (EMG)/nerve conduction velocity (NCV) studies are often non-diagnostic. Clinical suspicion and careful examination are pivotal to not overlooking this diagnosis; examination for RTS (including palpation of the course of the PIN under the brachioradialis, resisted supination of the forearm, and resisted extension of the long finger at the metacarpophalangeal joint) should be performed at every examination of a patient with the working diagnosis of LE. Other more distinct diagnoses to be ruled out include primary osteoarthritis of the radio-capitellar joint, collateral ligament sprain or instability, fracture, osteochondritis dissecans, and even cervical nerve root compression.
17.4 Surgical Indications
The primary indication for lateral epicondylar debridement is request for surgery by a patient who has demonstrated commitment but has failed to respond to 6 to 12 months of nonoperative treatment of LE.
17.5 Surgical Techniques
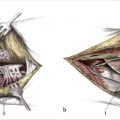
Regardless of one’s surgical approach, the basic tenets of successful surgical treatment of LE are release and debridement of the ECRB origin and fascia. The two most widely used approaches, open and arthroscopic, are worthy of consideration and comparison, because they have similar high rates of success and better functional outcomes than percutaneous release. 4 The percutaneous technique will not be discussed in this chapter.
17.5.1 Arthroscopic Debridement
Proponents of the arthroscopic approach suggest the advantages as primarily being able to identify and treat intra-articular pathology, such as osteochondritis dissecans (OD) and capsular plicas. However, one would expect the diagnosis of OD to be borne out before surgery. With regard to posterior radio-capitellar capsular plicas, there is no clear evidence that resecting this tissue, alone or in combination with debridement of the ECRB origin, improves outcome satisfaction in patients treated with surgical arthroscopy. 5 There are some claims in the literature that arthroscopic technique has a lower risk of complications and quicker return to work than open lateral epicondylar debridement. 6
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


