11 Laser Resurfacing with an Emphasis on Fractionated Technologies
Key Concepts
Fractionated carbon dioxide laser resurfacing has a quicker recovery than carbon dioxide laser resurfacing.
These technologies can be used for treatment of photodamaged facial skin, rhytids, lentigines, and dermal elastosis.
Although less frequent than after traditional resurfacing, complications can occur.
Any surgeon who performs fractional resurfacing should be prepared to diagnose and treat complications.
Introduction
Ablative laser skin resurfacing techniques emerged in the mid-1990s amid great fanfare and enthusiasm by the cosmetic practitioning community. The first lasers were high-energy, pulsed carbon dioxide (CO2) devices. They produced dramatic clinical results in the treatment of photodamaged facial skin, rhytids, lentigines, and dermal elastosis. Their drawbacks came in the form of prolonged recovery and risk of potential complications, which eventually made them less attractive treatment options.1 This spawned the development of nonablative devices, which solved the issues of prolonged recovery and treatment tolerability, but with less optimal clinical results.
Because of this limited efficacy, a new category of lasers was developed, fractional lasers. The first fractional lasers were nonablative. These were soon followed by ablative fractional lasers. The fractional ablative lasers bridge the gap between full ablative resurfacing and nonablative lasers. They provide clinically significant results with increased tolerability, lower risk of complications than ablative resurfacing, and minimal recovery time.2
Background: Basic Science of Procedure
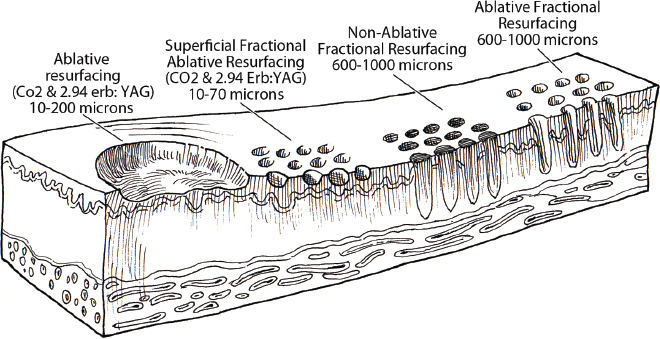
Fractional photothermolysis has revolutionized the entire field of laser skin resurfacing by providing significant improvement in clinical results with minimal posttreatment recovery and complications. This concept of fractional photothermolysis was first coined by Manstein and colleagues in 2004.3 The fractional technique differs from full ablative modalities in that ablative microcolumns are created with intervening skip zones of intact skin. These skip zones allow for adjacent heat dissipation during resurfacing and create the opportunity for horizontal wound healing. These columns are created in the epidermal and dermal layers to a controlled depth, width, and spacing ( Fig. 11.1 ). This is in contrast to devices that ablate the contiguous skin surface to a given depth. By ablating only columns of tissue, the healing is more rapid, and the potential for adverse effects, such as new dyschromia, infection, scarring, and prolonged erythema, is diminished. The small surface area of each “micro-wound” also results in rapid healing from the keratinocytes in the surrounding untreated skin.4
The fractional laser devices available today can be broken down into two types: ablative and nonablative. The ablative devices include CO2 (10,600 nm), yttrium-scandium-gallium-garnet (YSGG; 2,790 nm), and erbium-doped yttrium-aluminum-garnet (Er:YAG; 2,940 nm) lasers. The chromophore or target for these lasers is water in the epidermal and dermal skin layers. These high-energy lasers instantly heat the water, causing vaporization of the treated tissue with each pulse. This creates wound columns that can initially have some bleeding, serous drainage, and swelling lasting approximately a week or until reepithelialization is complete. The duration of erythema postfractional ablative resurfacing varies, but it typically lasts from 3 to 7 days.
The nonablative fractional lasers also target tissue water, but without causing an ablative wound. These include 850 to 1,350 nm infrared, 915 nm, 1,440 nm neodymium-doped yttrium-aluminum-garnet, and 1,540 and 1,500 nm erbium lasers. The laser zones created are coagulative in nature, with no epidermal ablation. Recovery is usually more rapid when compared with ablative modalities, and there is a lower risk of adverse events as already mentioned.5 These advantages are counterbalanced by less significant improvements in clinical outcomes, and multiple treatments may be required to achieve the desired results. Longer-wavelength nonablative fractional lasers can be used to treat some conditions in patients with higher Fitzpatrick skin types, such as melasma and scars. Ablative fractional lasers are usually not used to treat these conditions in patients with higher Fitzpatrick skin types.
Pertinent Anatomy
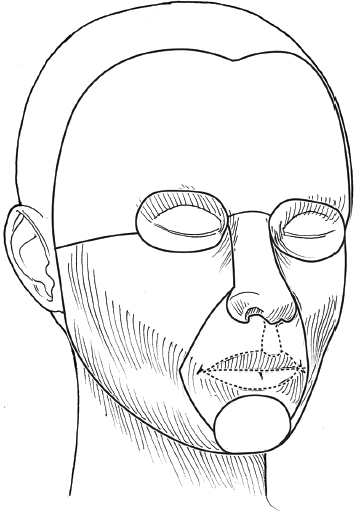
The anatomical subunits of the face are an important concept in all cosmetic procedures of the face ( Fig. 11.2 ). Knowledge of these helps guide the physician when deciding on a segmental area of resurfacing versus a full-face procedure. If a segmental resurfacing of the face is planned, such as rhytids in the perioral or periorbital regions, care must be taken to resurface the entire subunit for proper blending. Also, certain areas of the face can be more prone to scarring, such as the malar prominence along the jawline. Often, the subunits are drawn on the face prior to resurfacing to help guide the practitioner. The authors prefer not to resurface individual facial subunits, but perform a full facial resurfacing encompassing all subunits for balance and blending. The concern, even with fractional ablative resurfacing, is that there may be a noticeable difference if only a subunit is treated. Therefore, if segmental resurfacing is planned, we prefer to resurface at least the entire lower or upper two thirds of the face.
Skin type is also an important variable to consider before a resurfacing procedure. The Fitzpatrick skin typing is based on sun reactivity and tanning response to categorize an individual′s skin (see Table 6.4 ). Skin types I through III are usually considered resurfacing candidates because they have less pigmentation, and hence, less chance of dyschromia. However, a Fitzpatrick III skin type with any olive tones to the skin may be at a greater risk for dyschromia. The authors do not routinely perform ablative fractional resurfacing on patients with Fitzpatrick skin types V and VI. Patients with Fitzpatrick skin type IV can have significant variation in skin tone. The authors only perform fractional ablative resurfacing on these patients if they have lighter skin tones.
Patient Selection
One of the most important steps in the decision to perform a cosmetic procedure is proper patient selection. Several key points should be addressed in discussions with the patient prior to the procedure: (1) patient′s concerns; (2) pertinent medical history; (3) physical examination; (4) treatment options; (5) managing patient expectations; and (6) discussion of the procedure, associated risks and complications, and after care.
These obviously apply to every procedure the authors perform, but some specifics for laser resurfacing need discussion. The first step in the evaluation is the patient′s concerns. It is often helpful to have patients stand in front of a mirror with bright lighting and point out the areas on the skin they would like addressed. This creates a general cosmetic skin “wish list” that helps the practitioner understand the patient′s desires. This commonly includes rhytids, acne scarring, dyschromia, lentigines, rosacea, and actinic changes.
During this dialogue, a thorough evaluation of the patient′s skin should be performed. This includes evaluation of elasticity, pigment, texture, laxity, thickness, scarring, actinic change, and neoplastic processes. All cosmetics should have been removed prior to this portion of the examination. In addition, a full facial examination should be undertaken with focus on areas of concern for laser resurfacing, such as previous surgical and laser procedures, skin cancer resections, radiation therapy, isotretinoin (Accutane, Hoffmann-La Roche, Nutley, NJ) usage in the last year, or history of scar or keloid formation. Patients with a history of radiation therapy, isotretinoin, scleroderma, or burns can have damage to the adnexal structures of the skin, which are vital to skin healing because reepithelialization is initiated from within these structures. The authors recommend a 12-month waiting period after cessation of isotretinoin before resurfacing. Specific attention to the periorbital region and any history of blepharoplasty is recommended because even a slight lower ectropion or lid contraction can be greatly worsened by resurfacing. This can be evaluated by having the patient look upward while opening the mouth, which will reveal retraction or loss of lid elasticity.
The purpose of the initial patient evaluation is to gain a clear understanding of the patient′s expectations so that they can be managed accordingly. It is important to explain the expected result and that results vary from patient to patient. Photos of similar patients before and after the procedure help educate the patients on expected changes. Showing staged photos of patients on immediate postprocedure days to demonstrate the healing and appearance during this period has also proven helpful.
Technical Aspects of Procedure
Preoperative Preparation
All patients are instructed to avoid sun exposure for 4 weeks before resurfacing and are taught proper sun protection for the period after the procedure. Some surgeons do not advocate preconditioning for fractional resurfacing. For those who use preconditioning, it can be accomplished with application of retinoic acid 0.025% cream 3 weeks prior to speed reepithelialization.6 Hydroquinone can also be used 3 weeks prior to decrease the potential for postinflammatory hyperpigmentation, especially in darker skin types. This inhibits tyrosinase, thereby decreasing the formation and increasing the destruction of melanosomes within the melanocytes.7 If prophylactic antibiotics are used, they are usually started 1 to 2 days before the procedure and continued until most of the reepithelialization has occurred. Antiviral therapy is generally started 2 days prior to the procedure and continued until reepithelialization has occurred. Preoperative photographs are also obtained consisting of a front view and right and left three-quarter lateral views.
Procedure Technique
Patients are asked to cleanse their face before coming in for the procedure and are advised not to apply any makeup, moisturizer, or other topical skin products after cleansing. Further skin cleansing can be performed prior to the procedure with mild soap or glycolic wash.
The type of anesthesia required for ablative fractional resurfacing can vary depending on the specific laser and the surgeon′s preference. The authors use a topical anesthesia regimen of 6% lidocaine and 6% tetracaine prior to the procedure. This is applied for 15 to 30 minutes. No occlusion of the topical anesthesia is used. It is then thoroughly removed. Because the laser′s chromophore is water, the face should be completely dry prior to starting the procedure. During the procedure, a cool air chiller is used. This regimen provides a good level of anesthesia, and the patients are comfortable. The authors have not found a need for oral sedation for this procedure or injection of any local anesthesia, but there is no contraindication to either if needed for patient comfort. If sedation is utilized, the patient should be carefully monitored.
Immediately prior to commencing the procedure, standard laser safety precautions are undertaken. These include, but are not limited to, blocking of any windows so light cannot go through them and immediate availability of water, a fire extinguisher, and eye protection for the patient and the staff. Staff eye protection should be designed for the type of laser that is being used. The patient′s eyes should be covered with metal eye shields, either external or corneal types of shields. Plastic eye shields are not used because there is a risk of melting if struck by the laser.
A multitude of lasers exist for fractional resurfacing. As of this writing, there are no split face studies that clearly demonstrate the superiority of any one fractional resurfacing laser. The first author (LMD) uses a Matrix fractional CO2 laser (Sandstone Medical Technologies, Homewood, AL). Some patients have extensive superficial actinic changes of their facial skin. These patients may derive greater benefit from combined laser treatment with a fractional CO2 laser and superficial erbium laser treatment. Two separate laser devices can be used for this or they may be available in the same laser box, such as in the Cortex laser.
The settings used for any given laser vary depending on multiple factors. These include the physician′s laser experience and preference, the patient′s and physician′s goals for the treatment, the recovery time and recovery experience the patient is willing to undergo, potential risk factors for both systemic and local healing problems, and the patient′s age and skin thickness. Although the authors rarely do this for fractional resurfacing, if there is any question about the effects of a planned laser treatment, limited test spots can be performed and complete treatment deferred until the results of the test spots are evaluated. Additionally, if during treatment, either the patient′s experience or the effects of the laser vary from what was anticipated prior to the procedure, the procedure should be interrupted and an evaluation should be performed as to whether to alter or continue the procedure.
The following settings are those used by the first author (LMD) when treating patients with the Sandstone Matrix laser. With this laser, the surgeon has the ability to control many aspects of the laser process, including density, pulse duration, and fluence. The density of the microspots determines how close the laser ablation columns are on the skin surface. It can also be viewed as the percentage of the skin surface area that is treated. Pulse duration represents the pulse width or tissue ablation time. Laser power, represented in watts, correlates directly with the laser fluence.
All resurfacing is done in continuous-wave mode for fractional ablation. The pattern is generated in the handpiece and can be used in differing sizes and shapes depending on the surgeon′s preference and area being treated. These settings or techniques may not apply to other laser devices. Before using a laser, check with the manufacturer for recommended settings and techniques Video 11.1.
The laser is positioned at the patient′s side with the laser arm manipulated by the physician. The first author frequently uses a power of 21 to 23 W, density of 0.8 mm, and duration of up to 3 msec. These settings are not universally used by all treating physicians on all patients. The first author takes care to cover each subunit with a uniformly nonoverlapping square beam pattern beginning at the forehead. Care is taken to feather into the hairline for completeness. The second author (PJC) does not treat by subunits. Rather, he prefers to treat at least the lower two thirds of the face and, depending on the clinical findings, treat or omit treatment to the forehead region. An air chiller is also employed at the time of resurfacing to increase patient comfort. Most physicians use a smoke evacuator to remove the laser plume. Surgical masks with 0.1 µm pore size are also frequently worn by the physician using the laser and any other staff in the procedure room.
If resurfacing is performed in the periorbital area, milder settings should be used. The author does not resurface the skin of the upper eyelid below the upper eyelid fold. This is particularly important because fractional CO2 laser resurfacing can have a significant penetration depth.
The number of passes that are made and the settings for each pass vary between treating physicians and the patient′s particulars. If a second pass is performed, it should be performed starting over at the area that was first treated so that the dermis in this area has had time to cool while subsequent areas were treated. Furthermore, the fractional pattern of the second pass should not overlap the first pass to avoid double pulsing any area.
Resurfacing will, on occasion, extend into the neck and décolleté area. This can be done quite effectively with fractional resurfacing, but the laser settings must be adjusted. Moving to a lower power (16 to 18 W), decreasing density to 1 mm and lowering duration to 1 msec has proven safe and effective in this area for the first author. The neck and décolleté area have a lower sebaceous unit (adnexal structure) count in comparison to the face, a different blood supply, and a greater tendency for scarring. The lower settings are used to allow for these differences. Only one pass is made in these areas. If treated, these areas should be treated carefully because significant scarring has been reported in the cervical region after fractionated resurfacing.8
Two areas that warrant further discussion and caution on the face are the infraorbital and mandibular ridge regions. The skin of the infraorbital region is significantly thinner than the surrounding facial skin. This places it at higher risk for hypertrophic scarring and ectropion formation.9 Care should be taken in this area with lowered passes or energy settings, especially when laxity or previous surgery is noted. Similarly, the skin of the mandibular ridge is prone to hypertrophic scarring, so fewer passes, lower power, or lower density may be warranted in this area.
The skin will have a patterned appearance after fractional resurfacing with the residual of the vaporized epidermis and dermis at each of the microcolumns. It is not necessary to remove this. Pinpoint bleeding may also be noted in some areas immediately after the procedure or the evening after the procedure. This can occur when the fractional resurfacing extends into the level of the dermal plexus of vessels.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


