10 Intense Pulsed Light (with and without Photodynamic Therapy)
Key Concepts
Intense pulsed light (IPL) is similar in clinical effect to a variety of medical lasers.
IPL can be used to treat a wide variety of skin conditions.
IPL can be used for photodynamic therapy (PDT).
The combination of IPL and PDT may provide enhanced results for some conditions.
Introduction
Goldman and Eckhouse first described intense pulsed light (IPL) for use in medical therapy in 1990.1 Since that time, IPL has undergone multiple transformations to become the technology used commonly today. IPL devices use a xenon flashlamp to generate an intense polychromatic pulse of light energy in the spectrum of 400 to 1,300 nm. This polychromatic light can then be passed through various cutoff filters to eliminate undesired portions of the spectrum, yielding a band of wavelengths for clinical use. The concept of selective photothermolysis, as proposed by Anderson and Parrish,2 states that a target tissue has a particular absorption curve, and that this curve can be exploited to cause thermal damage of the target tissue without damaging surrounding tissues. This concept was originally proposed for laser tissue interactions, but it is also applicable to IPL.
The major difference in the two technologies is that laser light energy is monochromatic (1 wavelength, such as 1,064 nm) versus polychromatic (such as 480 to 550 nm) for IPL. Tissue absorption curves are not monochromatic, and nature has no requirement for light to be monochromatic for biological interaction. There are advantages and disadvantages to the use of polychromatic as opposed to monochromatic light. Monochromatic light will more accurately target a limited part of the tissue chromophore′s spectrum and may be less likely to cause collateral damage and hence side effects. However, polychromatic light can be used to treat a wider variety of skin conditions with a single device. IPL has been used successfully to treat several different skin conditions and lesions.3 This chapter focuses on the common applications of this technology in a facial plastic surgery practice.
Photodynamic therapy (PDT) is a group of therapies utilizing certain chemicals that are taken up by living cells and can then undergo molecular alteration when exposed to light energy, typically transforming them into metabolically active molecules. In its most basic form, PDT consists of any treatment that uses light energy to activate a chemical for medical treatment. Early treatments date back thousands of years to treatments for vitiligo used by the Egyptians.4 The current commonly used PDT chemical, aminolevulinic acid (ALA), was introduced into clinical practice in 1990 by Kennedy et al.5 Although ALA PDT has been used for a multitude of clinical problems, it is still not commonly employed in everyday practice. The focus here is on the application of PDT in a facial plastic surgery practice.
Patient Selection
The approach to the patient is similar when considering any light-based treatment: correct diagnosis of the condition, assessment of the individual′s skin type, and evaluation of potential complicating factors, such as medical conditions. Diagnosis of many lesions is possible by examination and history alone, but a biopsy should be considered for any lesion lacking a clear diagnosis. This is particularly true for pigmented lesions. Medical conditions that would preclude the use of IPL include conditions resulting in photosensitivity, pregnancy, breastfeeding, photosensitizing medications, and current oral retinoids. Relative contraindications include diabetes, coagulopathies, previous problems with IPL or light-based therapy such as pigmentary alterations, implants in the treatment area, and presence of a pacemaker. If the patient has a history of herpes simplex in proximity to the treatment area, antiviral prophylaxis should be considered.
IPL can be used to treat individuals with any Fitzpatrick skin type, but the darker skin types are much more difficult to treat and require particular caution. Tanned patients or patients with a history of postinflammatory hyperpigmentation will also require caution. Test spots are recommended for all patients at the initiation of treatment but are clearly advisable for patients with type II or darker skin. Test spots should be placed in a location with skin color and UV exposure similar to those of the area to be treated. Careful recording of the exact location of each test spot and the associated treatment parameters is mandatory. Assessment should be made of the immediate response to the test spot, and treatment parameters adjusted as necessary and repeated. The test spot(s) are evaluated at 4 to 6 weeks for pigment alterations or lack of effect and treatment parameters selected accordingly, or another series of test spots may be performed.
Once treatment parameters are selected, the areas to be treated are assessed for obstacles, such as hair, tattoos, and pigmented nevi. Hair will need to be shaved, and the patient should be informed that hair growth in the treatment area may be affected by the treatment. This may be problematic in the male beard or scalp in either sex. Hair loss may be permanent but is usually temporary. Nevi or tattoos may be covered with a white, damp, similar-sized piece of paper or cloth.
Pain associated with IPL treatments, while universal, is not typically severe, and if the patient complains of significant pain, one should reassess treatment parameters for overfluence. Some patients are less tolerant of treatments, and topical anesthetic creams may be used. Care should be taken in the application of these so as to avoid any potential for overdose with transcutaneous absorption. There have been several reports of lidocaine toxicity associated with the use of these topical agents in this setting. Cooling the skin with ice, chilled contact gel, or refrigerated air delivery devices such as the Zimmer Chiller (Zimmer Medizinsysteme GmbH, Ulm, GE) can also be helpful. Most devices have an integrated cooling tip that can be adjusted to the desired temperature.
After the treatment is complete, patients must avoid UV exposure for 4 weeks. Most patients will require more than one treatment, and this is discussed before treatment is started. For lentigines and photodamage, one or two treatments are typically sufficient, whereas vascular lesions will often require five or more treatment sessions. Hair removal will require more than five in almost all patients and many more in darker-skinned individuals. Typically, a minimum of 4 weeks between treatments is recommended, and in the case of hair removal, after the initial series of three or four monthly treatments, it is recommended to wait 2 to 3 months between treatments.
In selecting patients for PDT, all of the same considerations for IPL also apply to PDT, with a few additional ones. In general, PDT is most effective for photodamage and lentigines in patients with Fitzpatrick type I and II skin. Contraindications to PDT are disorders that cause increased photosensitivity, porphyria, and the patient′s current use of photosensitizing medications. PDT is also contraindicated in patients who cannot comply with UV avoidance for 48 hours after therapy. The discomfort associated with PDT is mildly greater than that with IPL alone, and the posttreatment sequelae of erythema, edema, and crusting are more pronounced.
Once the decision has been made to use IPL, a thorough discussion and documentation of the risks and benefits must take place. Specific detailed consent forms listing both common and uncommon posttreatment problems are helpful. The discussion should include both the expected posttreatment course of erythema and mild edema as well as the possibility of blistering, crusting, bruising, pigmentary alterations, burns, scars, and possible lack of effectiveness necessitating alternative therapy.
Technical Aspect of Procedure
Intense Pulsed Light
IPL devices can treat multiple types of lesions, which makes IPL an attractive first choice for light-based technology for many practitioners. It is challenging to select an IPL unit because there are multiple models available, most of which are stand-alone, but many are part of a multidevice platform that may contain a wide variety of other lasers or laser-like devices. The marketing for medical lasers is designed to convince potential customers that by purchasing a laser (or other device) they will be able to attract new patients to the practice. Unfortunately, this is often overstated. One must carefully appraise the potential clinical uses in one′s practice when considering these devices in general. Comparison of all the units available is not readily possible and is a moving target at best because new devices are introduced every year if not more frequently. In general, it is important that the IPL device have adequate ability to generate a stable square-wave pulse at the desired wavelength and fluence. This is dependent on the xenon light source and the capacitor bank that supplies the current for the flash. In other words, the device must be adequately powered to produce a constant current to the flashlamp so that power is not lost during the generation of the entire pulse. This is particularly important when multiple pulses are used back to back in “stacking.” Several device manufacturers also couple the light energy with other forms of energy, such as radiofrequency current. Whether or not this is important clinically is still debated.
The xenon light source of each IPL unit will have a designated lifespan that may range from 200,000 to several million pulses. The handpiece or treatment head contains the flashlamp as well as the light guide and cooling system and is susceptible to more wear and tear than other parts of the device. Almost all IPL devices have a sapphire contact crystal and require coupling to the skin with a gel for adequate function. The crystal may break or otherwise become nonfunctional, so a warranty or service contract should be considered when purchasing a device. One would want to examine the history and stability of the device maker as well as the reputation of the product. Although it may seem financially attractive to purchase a used device, the buyer should beware of the fact that most manufacturers will require the purchase of a service contract to work on used equipment, and this may offset some of the savings in the used device market. It is strongly recommended that several models be used in the office for a trial period before the decision is made to purchase.
The size of the contact crystal and treatment spot is another consideration because a larger surface area will allow the operator to cover more area with fewer pulses. However, too large a contact head may prove difficult to use in tighter spots, such as the upper lip. Larger spot sizes also require more power to deliver the fluences needed. The ability to adjust both wavelength, fluence and pulse width is critical to obtaining maximum effect from an IPL unit. Many units have preset parameters for treating specific conditions and skin types that are helpful for less experienced users, but the ability to adjust the settings is equally important as one gains experience. Many units now allow for “stacking” of pulses, which is the coupling of pulses back to back. Integral cooling of the tip is a common and important feature of almost all machines. Essentially all IPL units require the use of a gel, such as standard ultrasound gel, for optical coupling to the skin. This gel can be prechilled to add additional cooling if desired.
Routine photodocumentation is advisable before, during, and at the completion of a series of treatments. Documentation of Fitzpatrick skin type in the medical record is also essential. It is also wise to document the lack of tanning in the treatment area, as well as the discussion of the importance of UV protection after treatment.
Safety of both the patient and the treating professional is of paramount importance in all light-based therapy. The most easily injured organ is the eye due to the high pigment content, and opaque protective eye shields are used for the patient. Any treatments close to the eye must be very carefully delivered so as not to move the shields. The author believes the best ones for this application are metal, and they can be obtained from multiple vendors and are easily cleaned and reused. Protection of the treating professional′s eyes is more difficult. The broad spectrum of IPL requires very dark green lenses for protection. One should only purchase and use lenses labeled for IPL use. These lenses can pose some difficulty in assessing treatment end points and may have to be removed for adequate visualization of the biological response between treatments. There is no readily available solution to this issue.
Pigmented Lesions
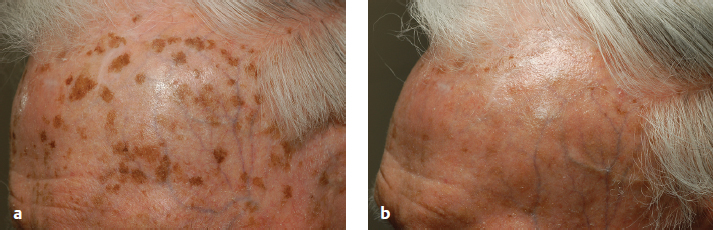
IPL can be an effective treatment for superficial pigmented lesions, particularly solar lentigines ( Fig. 10.1a,b ). As mentioned previously, the correct diagnosis is critical in all uses of IPL but particularly so for pigmented lesions. Biopsy should be considered for any lesion if the diagnosis cannot be made with a high degree of certainty. IPL is not effective for melanocytic nevi or seborrheic keratoses. Although there are several reports of the treatment of melasma with IPL,6 in general IPL is not very effective for treating melasma.
Lentigines, in general, are often a component of photodamaged skin, and in this situation IPL can be a very effective tool for clearing a larger area. For an isolated lentigo, a white piece of paper or plastic with a fenestration similar to the size of the lentigo can be used to shield the surrounding skin and increase the effectiveness of the treatment. Most lentigines will respond to a single treatment episode, and multiple treatments are not usually required. Darker lentigines respond better than lighter ones,7 and some authors find a Wood′s light useful to identify lesions more likely to respond, but with some practice it is not too difficult to identify lentigines that have a high rate of response. With IPL treatment, the typical immediate response for a lentigo is mild erythema and edema with some darkening of the lesion after treatment, progressing to significant darkening over 24 hours Video 10.1. Treatment parameters vary somewhat between IPL units, but in general a 560 to 590 nm filter is used with pulse duration of 5 to 10 msec and fluence of 30 to 40 J/cm2. If pulses are to be stacked, a delay of 25 to 40 msec is used. Again, test spots are recommended at several settings before treatment parameters are chosen.
After delivery of the selected treatment, the coupling gel is removed and the area inspected. A typical response is immediate darkening of the lesion followed by mild erythema and edema at the periphery of the lesion. If this is not noted, the area is re-treated at slightly higher fluence. Once the desired effect is obtained and the treatment is complete, a bland moisturizer with a sunscreen is applied. As mentioned earlier, the treatment is not painless, but it is well tolerated without topical anesthesia by most patients. The use of the cooling tip before delivery of the pulse, and immediately after, can be helpful in increasing comfort levels. If there is significant pain, one should suspect a too-high delivered energy level (overfluence). In this case, if the skin reveals more than mild erythema, immediate cooling should be applied for several minutes. The patient should be instructed to return if there is any evidence of blistering or crusting.
If the lesions revealed the expected response as already described, one can expect the lesion to darken further over 24 hours and begin to flake off at 7 to 10 days, revealing a mild erythema beneath that typically resolves in less than a week. UV precautions are recommended for 30 days after treatment. One can expect recurrence of many of the successfully treated lentigos over time, typically several years. This is somewhat dependent on the individual′s skin type and UV exposure, with lighter skin types with more UV exposure faring worse.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


