28 Wrinkle Reduction with Nonablative Lasers
Nonablative laser treatments for wrinkle reduction (where the term lasers* refers to both lasers and intense pulsed light devices) are aimed at heating the dermis to cause mild injury, while leaving the epidermis intact. A reparative healing process ensues after treatment with collagen shrinkage and synthesis of new collagen and extracellular matrix, referred to as dermal collagen remodeling.1,2 Dermal thickness is increased and the skin is smoothed, resulting in clinical reduction of wrinkles. In addition to wrinkle reduction, collagen remodeling effects with nonablative lasers can also result in reduction of depression scars, pore size, and rough skin texture.
Laser Principles and Devices Currently Available
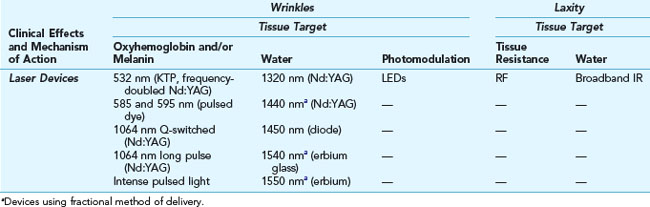
The mechanism by which most nonablative lasers effect collagen remodeling and wrinkle reduction is through focal thermal injury to the dermis while avoiding epidermal injury. Thermal injury can be induced through energy absorption in the skin by melanin, oxyhemoglobin, and/or water chromophores utilizing the principle of selective photothermolysis (see Chapter 19, Aesthetic Principles and Consultation).3 Other methods of inducing thermal injury include using radio-frequency energy, where tissue resistance to applied current heats the dermis. Some technologies utilize fractional methods of delivery that enhance the depth of laser penetration into the skin. Nonablative wrinkle reduction technologies can be broadly classified according to their clinical effects of wrinkle reduction or improvement in skin laxity, and this may be further refined based on the mechanism of action of the technology (see Table 28-1).
Wrinkle Reduction
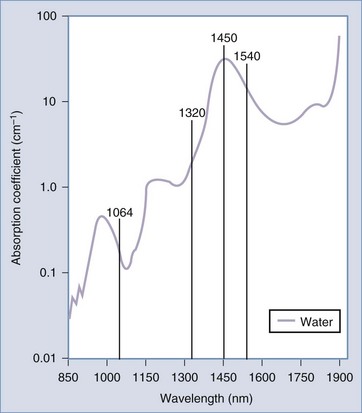
Many of the lasers used for nonablative wrinkle reduction target the water chromophore in tissue, including infrared (IR) wavelengths of 1320, 1440, 1450, 1540, and 1550 nm (1064 nm is also an IR wavelength but has less affinity for water). Figure 28-1 shows these wavelengths superimposed on the water absorption curve. By heating water, thermal energy is conducted to the dermal tissue, which stimulates the collagen remodeling process. All of these wavelengths have demonstrated clinical improvements in wrinkles.4–7
Some of the infrared lasers employ a fractional method of delivery (see Table 28-1), of which 1550 nm has the most data.8 Fractional lasers treat a portion or “fraction” of the skin by delivering laser energy in microscopic columns, called microthermal zones. Figure 19-10 in Chapter 19, Aesthetic Principles and Consultation, shows the pattern in the skin made by fractional laser devices. The untreated tissue between microthermal zones serves as a regenerative reservoir, which facilitates rapid wound healing.9 This type of treatment is termed nonablative fractional resurfacing. In addition to the collagen remodeling effects of wrinkle and scar reduction, fractional resurfacing with 1550 nm has also shown promise with reduction of dyschromic conditions such as melasma and poikiloderma of Civatte.10–12
Lasers that target oxyhemoglobin, melanin, and to a lesser degree water, such as 532 nm pulsed dye lasers (585 and 595 nm), and intense pulsed light devices (IPLs) have also been found to effect collagen remodeling and wrinkle reduction.13–15 However, the primary indication for these chromophore dependent lasers is reduction of vascular ectasias and/or pigmented lesions.
The Q-switched 1064 nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser was one of the first lasers to demonstrate nonablative reduction of wrinkles. Long-pulse 1064 nm Nd:YAG lasers are also used for reduction of wrinkles and results may be enhanced when combined with 532 nm.16–18 The long 1064 nm wavelength, as with other infrared lasers, allows for deep penetration to the dermis, which is desirable for collagen remodeling and, because it has little absorption by epidermal pigment, this wavelength is safe for all skin types. Studies with Q-switched 1064 nm lasers demonstrate histologic19,20 and clinical reduction of wrinkles, as well as other collagen remodeling effects, such as reduction of pore size, rough skin texture,21 and superficial acne scarring.22–24 Dermal collagen remodeling effects are due to both photothermal and photoacoustic vibration, which results from the inherent rapid, short (nanoseconds) pulses of Q-switched lasers.25 In addition to dermal remodeling, Q-switched 1064 nm lasers are also commonly used for tattoo removal,26 reduction of dermal pigmentation such as melasma,27–29 and reduction of fine dark hair.30 The diverse applications of Q-switched 1064 nm and other chromophore-dependent lasers offer a means to address many aesthetic skin complaints simultaneously.
Light-emitting diodes (LEDs) are a newer type of light-based device that emit a narrow range, or band, of wavelengths. They do not operate based on the theory of selective photothermolysis, but are instead based on the principle of photomodulation, whereby cellular activity is modulated through illumination with particular wavelengths of light.31 These devices have been used for mild wrinkle reduction32 and treatment of acne. Several LEDs are available that vary in wavelength and pulsing modes such as blue light devices (400 to 500 nm) which have superficial penetration, and red light devices (570 to 670 nm) which have deeper penetration. The main advantage of LEDs is their ease of use.
LEDs have also been used for skin rejuvenation as part of photodynamic therapy (PDT). PDT refers to selective tissue destruction through the use of a photosensitizing medication that is activated by a laser or light-based device (such as an LED or IPL).33 A topical photosensitizing medication such as aminolevulinic acid (Levulan®) is concentrated in particular tissues, such as sebaceous glands and actinically damaged cells. The photosensitizer is activated by a light source resulting in a cytotoxic reaction and destruction of the targeted areas.34 PDT is currently FDA approved for treatment of nonhyperkeratotic actinic keratoses, but is used off label to enhance the results with nonablative lasers for photorejuvenation and wrinkle reduction.35–37
Reduction of Skin Laxity
Skin laxity is treated with two main types of technologies: broadband infrared and radio-frequency (RF) devices.38 The improvements in laxity are believed to be due to collagen contraction initially, and later to collagen synthesis.39 Broadband infrared devices (such as the Cutera Titan™) emit wavelengths ranging from 1100 to 1800 nm with long pulse widths (of several seconds). Radio-frequency devices (such as Solta Thermage™) employ rapidly alternating current that creates heat when applied to the skin because of the skin’s resistance to the flow of current. Tissue heating with RF devices is controlled by several factors, including the type of electrodes used (e.g., monopolar or bipolar), fluence, and cooling times. These technologies have been shown to improve laxity in many areas of the body including the periocular region, nasolabial folds, jowls, neck, and abdomen.40–45 In addition to treatment of wrinkles and skin laxity, RF devices are also used for cellulite reduction.46 RF treatments have traditionally been associated with more discomfort than IR treatments, however, new techniques utilizing multiple passes with lower fluences have improved tolerability.47
Patient Selection
Patient selection for wrinkle reduction treatments with nonablative lasers is based on the degree of wrinkling present and patient expectations. Patients with mild to moderate static wrinkles and laxity (Glogau types I through III) are appropriate candidates (see Chapter 19, Aesthetic Principles and Consultation, for a description of Glogau types). Patients with deep static wrinkles and/or severe laxity (Glogau type IV) and those who desire more rapid and dramatic results may be better candidates for more aggressive procedures such as ablative laser resurfacing or surgery.
Products Currently Available
See the Resources section at the end of the chapter for a list of laser manufacturers.
Advantages of Nonablative Lasers for Wrinkles
Anatomy
Wrinkles result from many factors including skin changes with epidermal hypocellularity, loss of dermal matrix components including collagen, glycosaminoglycans, elastin, and atrophy of subcutaneous adipose tissue. Thinning of the skin combined with repetitive contraction of underlying musculature can etch wrinkles into the skin to form static lines.48
Nonablative laser treatments are aimed at reducing mild to moderate static wrinkles. Most of these technologies do so by producing papillary dermal injury, at an approximately 100 to 200 µm (0.1 to 0.2 mm) depth in the skin.49,50 Fractional nonablative laser treatments for wrinkles (e.g., fractional 1550 nm) penetrate up to 300 to 400 µm (0.3 to 0.4 mm).9 Nonablative lasers for laxity (e.g., RF lasers) penetrate to the reticular dermis, up to 1 to 3 mm.51
Procedure Preparation
Nonablative Lasers for Wrinkles: Steps and Principles
General Treatment Technique






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


