Chapter 42 Whipstitch-Post Tibial Fixation for Anterior Cruciate Ligament Reconstruction
Biomechanics
Elongation and Stiffness
The purpose of fixation is to hold the graft without allowing elongation from the fixation site until biological healing has occurred. Elongation can occur from slippage of the fixation device relative to the bone or slippage of the graft relative to the fixation device. Although stiffness has been much considered as an important attribute of ACL graft fixation devices, it is less important than elongation because it only represents the elasticity of the graft–fixation construct prior to the healing of the graft in the tunnel. For BPTB this is roughly 6 weeks. For soft tissue it is 8 to 10 weeks. After this period the stiffness of the fixation device or the extraarticular portion of the graft is no longer part of the load-bearing portion of the structure, which consists only of the intraarticular portion of the graft. In fact, a high-stiffness construct will tend to concentrate mechanical force on the graft–bone interface before graft incorporation has occurred, whereas a low-stiffness construct will dissipate graft strain through elastic deformation of the graft–fixation construct and potentially offer some protection to slippage or elongation at the fixation–bone interface. The WSP method relies on extratunnel cortical fixation and would be a lower-stiffness construct than an aperture-fixated construct because it is longer, if all else were equal. However, To et al1 have shown that the increase in stiffness produced by the use of cortical fixation is much greater than the reduction in stiffness from the greater length of the construct.
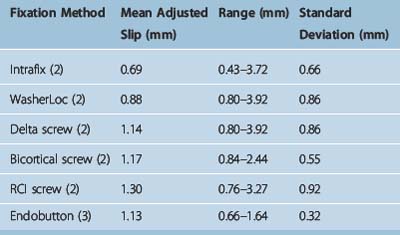
Clinically, grafts usually elongate as a result of cyclical loading, not catastrophic failure. Some of the lowest elongations yet recorded from cyclical loading were published in a recent study of six commonly used devices by Coleridge and Amis2 and are in the range of 1 mm after 1000 cycles. In a recent study we found elongation using WSP fixation to be unsurpassed by any of these fixation devices3,4 (Table 42-1). The standard deviation was also very low, indicating high consistency of the fixation results.
Indirect Versus Direct Fixation
Direct fixation holds direct purchase on the graft. Examples are interference screws and spiked ligament screw washers. Indirect fixation holds purchase through an intermediary substance. Tibial WSP fixation is in the indirect category, as is the fabric loop of Endobutton fixation. Both methods can be used effectively. However, indirect fixation has the added advantage of being able to accommodate a shorter graft. There is evidence that 15 mm5 or less6 is sufficient graft length in the tunnel to allow satisfactory healing. This is all that is needed for indirect fixation such as the WSP described here. Greater length is required for interference screw fixation to allow sufficient length of graft along the interference screw. Even more length is required if a spiked ligament screw washer is used on the tibial cortex because the graft must be long enough to extend out of the tibial tunnel.
Clinical Results
A recent meta-analysis of all HS and BPTB clinical series7 subdivided HS grafts into subgroups by fixation type. The subgroup with the highest stability rates used an Endobutton on the femur and primarily WSP tibial fixation. Of the six high-stability series with no graft failures, four used WSP fixation.8–11 Finally, the study with the overall highest stability rate also used WSP.8 Recently presented data from a series of five-strand hamstring grafts12,13 that used WSP fixation on both the tibia and femur with mean 8-year follow-up had the highest stability rates yet reported for a semitendinosus/gracilis (ST/Gr) graft.8 It should also be pointed out that these stability rates exceeded those found using BPTB from this same meta-analysis.
Morbidity, if the screw is carefully placed, is almost nonexistent. A 0% rate of screw removal due to patient irritation from the cortical screw post has been recently reported in a large series with 2- to 8-year follow-up.11
Surgical Technique
Suitable Tibial Screws
Many suitable products are available (Fig. 42-1). We use the Smith & Nephew 4.5-mm screw, which does not require a washer. The screw is best inserted with a 2.7-mm drill bit rather than the 2.4-mm bit supplied by the company. It should always be tapped. Most screws are 25 to 35 mm in length. Linvatec makes an excellent 6.5-mm screw that we used for years, which does require a washer. Arthrex makes a bioabsorbable screw that we would not recommend (see later discussion). Arthrex also makes a 4.5-mm screw for use without a washer and a 6.5-mm cancellous screw, which is used with a washer. This last screw, however, is used with a small, 2.5-mm, hexagonal screwdriver. In the past we had problems with screwdriver head breakage due to the smaller hexagonal size relative to the larger screw.

Bioabsorbable or Radiolucent Tibial Screws
Radiolucency
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


