Chapter 67 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction
A Review of the Current Literature
Anterior cruciate ligament (ACL) reconstruction is one of the most prevalent orthopaedic procedures, with more than 100,000 performed annually.1 The majority of these operations use autograft donor tissue, with hamstring tendons (either semitendinosus [ST] or semitendinosus with gracilis [ST/Gr]) recently gaining approval in relation to the traditionally favored bone–patellar tendon–bone (BPTB) graft. Historically, the BPTB graft has been advocated for a number of reasons, including its well-described regrowth phenomenon, which involves the reconstitution of its central third following harvest. However, supporters of hamstring grafts cite potential patellofemoral pain, patellar tendonitis, tendon rupture, and patellar fracture as possible disadvantages of BPTB use.2–5 In 1992, Cross et al reported the regeneration of the hamstring tendons following harvest, a notion that has been supported with increasing evidence in the literature.6 Overall, as a result of this regeneration of the harvested tendon, hamstring strength has been found to reach near-normal levels 1 year postoperatively. This regeneration is termed the lizard tail phenomenon. The validation of such a phenomenon may offer an additional advantage for the use of hamstrings in ACL reconstruction. This chapter will review and summarize the literature to date examining the morphological and functional regeneration of harvested ST/Gr tendons from a radiographic, functional, and histological standpoint. It must be noted that relevant studies are somewhat difficult to compare due to unavoidable differences in follow-up, rehabilitation protocol, and testing methods found in the literature. Additionally, some studies confer results following ST/Gr harvest, whereas others evaluate those involving only ST harvest.
Radiographic Studies
A number of studies have attempted to describe the morphological aspect of regeneration using the radiographic images of the ST and Gr tendons following harvest. These studies have provided information concerning the extent of regeneration, the location of the regenerate tissue, and the presence or absence of muscle atrophy. In the study conducted by Cross noted previously, magnetic resonance imaging (MRI) evaluation of four patients (6 months postoperatively) displayed tendonlike tissue extending from the hamstring muscle bellies to the medial gastrocnemius (Fig. 67-1).6 In this case, insertion appeared to be diffused into the medial popliteal fascia, but electromyographic examination revealed normal muscle activity and innervation patterns in the hamstring. Simonian et al similarly reported proximal insertion of the regenerate ST tendon.7 In contrast with common trends in the literature, however, no compensatory hypertrophy of the biceps femoris, semimembranosus (SM), or sartorius was appreciable when compared with the unaffected side.

A number of papers by Eriksson et al have reported MRI imaging of regenerate hamstring following harvest of the ST tendon. In the first (1999), they reported ST regeneration to the level of the proximal tibia in 8 of 11 patients evaluated 6 to 12 months postoperatively, whereas in the other three patients the remnant ST fused with the SM tendon proximal to the joint line.8 Those patients with regenerate distal ST demonstrated fusion of the ST and Gr approximately 30 mm distal to the joint line with insertion as a conjoint tendon on the pes anserinus. The authors suggested that the precise level of union is insignificant as long as it is distal to the joint line. The proximal cross-sectional area of the ST also differed between groups. This measure averaged 91% of the contralateral tendon in those with distal regeneration and 79% in those without distal regeneration. In a second study (2001), Eriksson et al evaluated six patients who ranged from 7 to 28 months following ACL reconstruction, using only the ST graft.9 MRI imaging displayed regeneration of ST tissue in five of the six patients to the pes insertion site, averaging approximately 30 mm distal to the joint line. The sixth patient had no evidence of a new tendon 24 months after surgery. Concurrently in 2001, Eriksson and Hamberg published another study in which patients underwent MRI between 6 and 12 months after ST harvest.7 In this case, 12 of the 16 patients displayed radiological evidence of ST regeneration in which the new tendon fused with the (nonharvested) Gr 10 to 30 mm below the joint line and inserted on the pes as a conjoined tendon. Although some ST atrophy was notable in all patients, significantly more was appreciable in patients without tendon regeneration. In those patients without regeneration, however, compensatory SM hypertrophy was more extensive.
Rispoli et al performed their study in a different manner, attempting to provide radiographic documentation of tendon regeneration in 21 patients at distinct time intervals ranging from 2 weeks to 32 months following ACL surgery using ST/Gr.5 However, they did not sequentially image any individuals. At the points shortly following surgery, fluid and edema in the tendon tracts were noted, and tendonlike tissue reached the superior patellar pole 6 weeks after surgery. Presence of the tendons below the joint line arose at variable intervals, arising anywhere from 3 to 12 months postoperatively. Papandrea et al also observed similar linear development in a study using sequential ultrasounds of 40 patients at 2 weeks, and 1, 2, 3, 6, 18, and 24 months after surgery using ST/Gr.10 This study documented a course of maturation proceeding from ill-defined hypoechogenic tissue early on to hamstring hypertrophy in the first year, before a distinct, well-defined tendon signal developed between 18 and 24 months. This study noted a more proximal insertion into the medial popliteal fascia than normal.
This process has been further documented by multiple other studies as recently as 2004. Nakamura et al used MRI and three-dimensional computed tomography (3D-CT) scans in a retrospective study assessing ST regeneration in eight patients, each a minimum of 2 years postoperative.11 In five of eight patients, distinct tendonlike tissue was observed running along the same course as the native hamstrings, the most notable difference being distal attachment to the medial popliteal fascia. In the remaining three subjects, the residual ST fused proximally into the SM muscle belly. The study apparently observed similar regeneration of the Gr, but an explicit description was not included. Tadokoro et al also imaged 28 patients with MRI at a minimum of 2 years following ACL reconstruction with ST/Gr.12 This study reported regeneration of 22 of 28 ST tendons and 13 of 28 Gr tendons, with no differences in cross-sectional area between surgical and contralateral knees. More importantly, they found that there was no correlation between morphological regeneration and peak flexion strength in high degrees of flexion (90 and 110 degrees) in both prone and supine positions despite less strength in affected limbs.
Williams et al also performed MRI on eight patients both preoperatively and at the point of return to sports (an average of 6 months after reconstruction using ST/Gr).13 Seven of the eight patients exhibited regenerate tendons; however, the majority of the tendons had not yet inserted on the tibia at the point of imaging. Overall volume of the ST and Gr muscles diminished by an average of 30%, and in contrast with Tadokoro’s study, this extent appeared to correlate well with the extent of tendon regeneration. Additionally, much like Eriksson’s study, compensatory hypertrophy of the SM and biceps femoris muscles was noted.
Nakamae et al also used 3D-CT to gain a better sense of the full-length morphology of the regenerate tissue by imaging 29 patients at various time points.14 A 3D-CT examination was performed in all patients preoperatively, 24 patients at 1 month, 8 patients at 3 months, 21 patients at 6 months, and 20 patients at 12 months postoperatively following ST harvest only. Although no patients had evidence of regeneration at 1 month after surgery, a regenerate tendon was detected in all but two patients at 12 months after surgery, with the regenerate tissue coursing as expected from the muscle bellies to the normal insertion site on the proximal tibia.
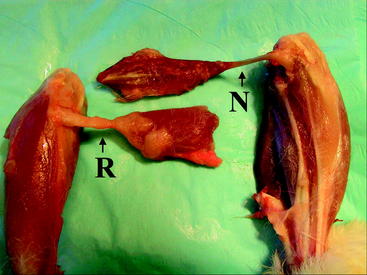
Although there is a perception that regeneration occurs almost universally, it is not an entirely predictable phenomenon. For reasons not fully understood, a small percentage of patients in a number of studies lack regenerate tendons. Notably, two studies by Eriksson and one by Hioki et al report 17%, 18%, and 45% of patients with failed regrowth, respectively.3,9,15,16 Additionally, among the population with evidence of regrown tissue, the regenerate tendon frequently ranges in size and diverges from the expected insertion site, inserting proximally and medially to the pes anserinus (Fig. 67-2). This varied insertion could have important biomechanical consequences that explain varied strength of knee flexion and internal rotation. A more proximal insertion shortens the tendon’s moment arm, inhibiting the muscle’s ability to flex the knee. Additionally, in the case of documented insertion on the medial popliteal fascia, a more lateral insertion hinders the hamstring muscles from generating internal torque and resisting external rotation of the tibia.
Functional Studies
Numerous studies have also examined hamstring strength following tendon harvest. Postoperative leg strength has been a concern since at least 1982, when Lipscomb et al published a retrospective evaluation of 482 cases involving either ST or ST/Gr harvest.17
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
Anterior Cruciate Ligament Reconstruction Utilizing the Rigidfix for Femoral-Sided Fixation
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


