Chapter 31 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Biomechanics
Numerous studies have analyzed the pullout strength and stiffness of this device.1–7 Much was made at one point about a so-called “bungee effect,” in which the device’s fixation on the cortex and not in the tunnel supposedly resulted in lower stiffness. However, it has subsequently been shown that the greater stiffness resulting from cortical anchorage dwarfs the slightly reduced stiffness from the greater length of the construct.7 Also, as described elsewhere in the text, stiffness has no bearing on ultimate stability. This is because the stiffness of all grafts is independent of their mode of fixation once tunnel healing has occurred at about 2 months postoperatively. After this time, load is borne by the healed fibers that connect the graft to the tunnel, not by the device. Because the fixation device is not load bearing after this time, its stiffness is irrelevant. However, even before that time, stiffness is less important because the stiffness represents only elastic deformation of the graft. It is only plastic deformation, not elastic deformation, that will result in greater ultimate clinical laxity. In fact, reduced stiffness, or greater elasticity, in the graft-fixation construct will diminish the forces that tend to displace the fixation device in cyclical loading. This reduction in stiffness diminishes these forces by partially dissipating them in temporary elastic deformation of the graft. Therefore, ultimately, stability may actually be enhanced by protecting the construct from plastic deformation or fixation device slippage while tunnel healing is occurring.
Clinical Results
In the largest meta-analysis of anterior cruciate ligament reconstruction (ACLR) autografts, the EB-hamstring combination was found to have the highest stability rates of any graft-fixation construct when paired with modern tibial fixation.8–14 Morbidity has been minimal.15–18 In our experience,8 the EB has proven to be extremely reliable. After 13 years of continuous use, as well as follow-up of more than 80% of all implanted EBs, we have had no graft failures (see Chapter 69). Approximately 86% of grafts have had IKDC normal stability. We have had no hardware complications and no displaced EBs, and we have not had to remove an EB.
Surgical Technique
Femoral-Tunnel Formation
Finishing the Femoral Tunnel
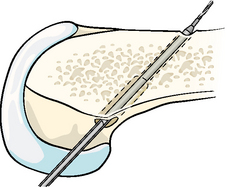
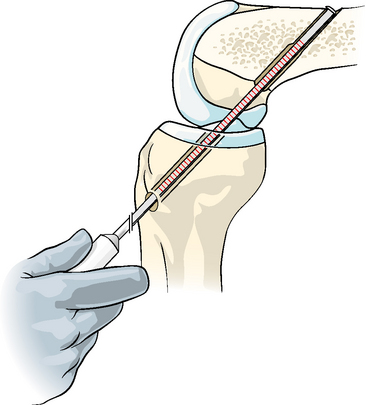
Once a satisfactory tunnel has been found, the laser pin is further drilled through the cortex. We observe the laser markings when giving way is achieved, which indicates the pin has burst through the cortex, so we have a good idea of the total channel length. Next, the appropriate acorn reamer is inserted over the pin. This is drilled nearly to the cortex, as measured from the laser pin. If high resistance is felt before the anticipated point is reached, drilling should be stopped to avoid breaking through the opposite cortex. Generally the acorn reamer will be drilled 1 to 2 mm shorter than the laser pin length indication of where the cortex was reached. The socket will usually be about 6 mm shorter than the total channel length. It must be within 9 mm of the length of the total tunnel to allow a 15-mm EB-CL to be used. This is because at least 6 mm of extra length is needed to allow a turning radius for the EB as it sits outside the femoral cortex (i.e., 6 + 9 = 15 mm). Once the socket is drilled, the acorn drill bit is withdrawn and a 4.5-mm bit is inserted and drilled through the outer cortex with the guide pin still in place (Fig. 31-1). After the 4.5-mm tunnel is drilled, the guide pin is removed with the 4.5-mm drill bit. Next, the long-depth gauge is used to measure the total channel length (Fig. 31-2). If it exceeds the socket length by more than 9 mm, the guide pin and then the acorn drill bit should be reinserted over the guide pin, and the socket should be drilled a little farther so that it is within 6 to 9 mm of the total length. If the far wall of the cortex is accidentally violated, this can be easily salvaged with an Xtendobutton, as will be described.
Preparing the Endobutton/Graft Construct
The EB-CL is positioned in the holder on the Graftmaster board. The graft is then passed through the fabric loop attached to the EB (Fig. 31-3). A violet #3–0 or 4–0 monofilament absorbable suture is then sewn across the graft (Fig. 31-4
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 EZLoc Femoral Fixation of a Soft Tissue Graft
EZLoc Femoral Fixation of a Soft Tissue Graft
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


