The diagnosis of alopecia and other hair-related disorders can be challenging. An appreciation of the newest diagnostic techniques and newly described entities can help clinicians to provide the best care for patients. This article focuses on advances in the histologic evaluation of alopecia. Also discussed are recent advances in the understanding of hair-related disorders that do not result in alopecia. Advances in the understanding of disease mechanisms can help in treating hair disorders that proved refractory in the past.
- •
In most cases, an alopecia diagnosis can be reached with either vertical or transverse sections.
- •
The HoVert technique for sectioning alopecia specimens is an ingenious method that provides vertical and transverse views of portions of a single scalp biopsy specimen.
- •
The Tyler technique has additional advantages.
- •
Large tufts of hair protruding from a common infundibulum (“six-packs” or “doll’s hair”) can be a clue to the quiescent phase of neutrophilic forms of alopecia, especially folliculitis decalvans and acne keloidalis nuchae.
Alopecia
Several recent articles have contributed to knowledge of alopecia and have refined the diagnostic criteria. Some have focused on practical questions of how to section biopsy specimens to optimize the diagnostic yield. The first portion of this article focuses on advances in the histologic evaluation of alopecia.
How to Section the Specimen When Only a Single Punch Biopsy is Received
In most cases, a diagnosis can be reached with either vertical or transverse sections. Vertical sections are superior for the diagnosis of scarring alopecia and comparable with transverse sections for alopecia areata. Transverse sections have advantages in the diagnosis of other forms of nonscarring alopecia. Combining the two maximizes the diagnostic yield. When only a single specimen is received, various techniques have been proposed to provide vertical and transverse sections from a single specimen.
The HoVert technique for sectioning alopecia specimens is an ingenious method that provides vertical and transverse views of portions of a single scalp biopsy specimen. The HoVert technique entails transecting the 4-mm punch scalp biopsy transversely, 1 mm below the epidermal surface, to create an epidermal disk and a lower portion. The epidermal disk is then bisected to provide vertical sections of the upper half of the specimen. On the slide, the lower portion of the specimen is viewed in transverse (horizontal) section, whereas the sections from the upper half are seen in vertical section to provide a higher diagnostic yield for such conditions as lichen planopilaris (LPP) that preferentially affect the follicular infundibulum and can be missed with transverse sectioning.
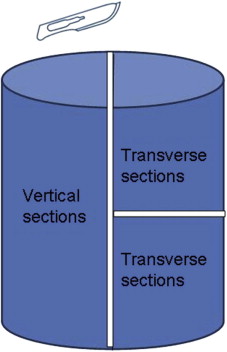
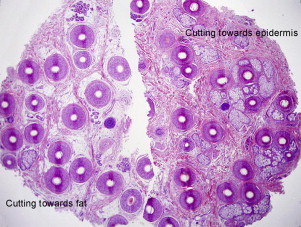
The Tyler technique is an alternate method in which the specimen is first bisected vertically, and then one-half of the cylinder is sectioned transversely ( Fig. 1 ). All sections are embedded together in a single cassette. The two resulting transverse half-moons are embedded side by side to create the impression of a single complete transverse section with an adjacent complete vertical section. An advantage of this technique is that it produces a full vertical section (from the stratum corneum to the subcutaneous fat) rather than vertical sections that show only the upper half of the follicle. Another advantage is the ability to view all levels of the dermis in transverse sections, because serial sections show progressively higher transverse sections in one half-moon and progressively lower levels in the other half-moon ( Fig. 2 ). The Tyler technique may be advantageous when a single specimen is received and the differential diagnosis includes such conditions as lupus erythematosus, central centrifugal cicatricial alopecia, or alopecia areata, where key histologic features are typically below the bisected level of HoVert specimens. However, it should be noted that because all portions of the specimen can ultimately be represented in serial sections with either technique, it may largely be a matter of individual preference. Both techniques have significant advantages over purely vertical or purely horizontal sectioning.
Tufting as a Clue to Neutrophil-Mediated Scarring Alopecia
Large tufts of hair protruding from a common infundibulum (“six-packs” or “doll’s hair”) can be a clue to the quiescent phase of neutrophilic forms of alopecia, especially folliculitis decalvans and acne keloidalis nuchae ( Fig. 3 ). Lymphocyte-mediated forms tend to produce smaller clusters of hairs. Large tufts can also be seen after burns and as physiologic tufting, especially in the occipital scalp, so the finding of six-packs must be interpreted in the context of the clinical presentation.

Lymphoma Presenting as Alopecia
Alopecia in mycosis fungoides and Sézary syndrome
Alopecia can be an important manifestation of mycosis fungoides and Sézary syndrome. A retrospective study of 1550 patients noted 38 patients with patchy, total-scalp, or universal alopecia. Thirteen (34%) of the 38 had patchy alopecia clinically identical to alopecia areata. Although alopecia areata is characterized by peribulbar lymphoid infiltrates, lymphocytes or eosinophils in fibrous tract remnants, pigment in fibrous tract remnants, catagen hairs, pigment casts, and dilated follicular infundibulae, mycosis fungoides is more likely to demonstrate epidermotropism of large angulated lymphocytes throughout the follicular epithelium, basilar tagging, and halos surrounding lymphocytes. Follicular mucinosis may be present. The histologic changes in Sézary syndrome are far more variable and can be nonspecific. The syndrome is best confirmed by the combination of clinical erythroderma and circulating Sézary cells.
Scarring alopecia in B-cell lymphoma
Primary cutaneous follicle center cell lymphoma of the scalp has recently been reported presenting as scarring alopecia. There is overlap at scanning magnification with lupus erythematosus presenting with prominent germinal centers. Careful attention should be paid to the symmetry and regularity of the lymphoid nodules, symmetry of the surrounding mantle zone, and presence or absence of tangible body macrophages. Both demonstrate follicles composed mostly of CD20 + centrocytes, but the lymphomas often demonstrate disruption of the CD21 + network of dendritic cells within the lymphoid follicles and wandering of BCL-6 + follicle center cells beyond the confines of the follicle.
Subtle Clues to the Diagnosis of Trichotillomania
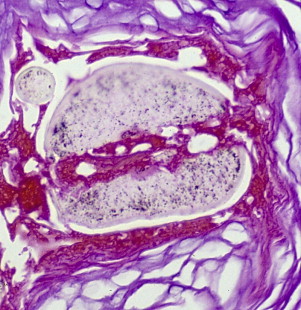
Histologic features of trichotillomania (trichotillosis) include empty anagen follicles, multiple catagen hairs, pigment casts in the follicular channel, and trichomalacia. Of these, the most specific finding is trichomalacia, which can produce striking findings, such as the “hamburger bun sign.” This involves a vertically oriented split in the hair shaft, containing proteinaceous material and erythrocytes, morphologically reminiscent of a hamburger in a bun ( Fig. 4 ). Degeneration of the hair fiber can take other forms, such as the “hot dog” sign ( Fig. 5 ).
Subtle Clues to the Diagnosis of Alopecia Areata
Helpful diagnostic signs in alopecia areata include the presence of peribulbar lymphoid infiltrates, follicular miniaturization, dystrophic follicles, catagen hairs, pigment incontinence in fibrous tract remnants, lymphocytes or eosinophils in fibrous tract remnants, and pigment casts within follicular channels. Several of these features overlap with other entities, and careful attention must be paid to the entire constellation of findings and the clinical presentation. Yellow dots have been noted on dermoscopy, which correspond histologically with dilated follicular infundibula, and this finding can help to distinguish alopecia areata from trichotillomania, telogen effluvium, and pattern alopecia. The finding has been likened to a Swiss cheese appearance.
Reflectance Confocal Microscopy
Reflectance confocal microscopy was evaluated in seven white patients with LPP or discoid lupus erythematosus involving the scalp. Discoid lupus erythematosus and LPP demonstrated spongiosis, exocytosis, interface dermatitis, periadnexal infiltration of inflammatory cells, dilated dermal vessels, and melanophages. In LPP, bright rims around the adnexal epithelium and dermal papillae were obscured by inflammatory cell infiltrates along a large front, whereas this is a focal finding in discoid lupus erythematosus. During therapeutic follow-up, marked reduction or absence of inflammatory cells at the level of the epidermis, upper dermis, and adnexal structures was considered evidence of complete remission. The authors concluded that reflectance confocal microscopy demonstrated promise in diagnosis and evaluation of therapeutic response.
Overlap Alopecia
Flares of LPP are commonplace after attempts at scar revision or hair transplantation. Progressive scarring alopecia secondary to LPP was recently described in the setting of follicular unit transplantation for androgenetic (pattern) alopecia, emphasizing the need to be alert for the presence of scarring alopecia superimposed on a background of pattern alopecia. LPP has also been reported after trauma from breakdancing. The resulting apical alopecia mimicked pattern alopecia.
Ethnic Variation in Alopecia
A study of scarring alopecia in Indian patients revealed 18 (49%) of 37 patients with a diagnosis of lupus erythematosus, 15 (41%) of 37 with a diagnosis of LPP, one patient with folliculitis, and three with alopecia areata. Important differentiating features for lupus erythematosus included epidermal atrophy, papillary dermal fibrosis, mucin, peribulbar inflammation, and haphazard spacing of scars, compared with LPP, which typically demonstrated a normal epidermis, peri-infundibular infiltrate, and regular spacing of scars. Twelve cases demonstrated total absence of follicles but could be classified based on the connective tissue changes, emphasizing the importance of dermal changes and elastic tissue stains in the diagnosis of alopecia (see later). Not surprisingly, patients described as “pseudopelade” clinically were most likely to show LPP on histologic examination.
In another recent histologic study of alopecia areata in Indian patients, the diagnosis was made on vertical sections in all 20 cases. The anagen/nonanagen ratio was 1:1.62. Miniaturization of follicles was noted in five (25%) cases. Peribulbar inflammation was noted in all the cases with a dominance of lymphocytes, and pigment casts were present in five cases. These findings suggest that clinicians had biopsied early lesions of alopecia areata.
According to a recent study, central hair loss in African American women does not seem to be associated with relaxer or hot comb use; a history of seborrheic dermatitis; or reaction to a hair care product, bacterial infection, or male-pattern hair loss in fathers of subjects. Future studies need to address the influence of recall bias. I myself have had patients flatly deny ever having straightened their hair, only to have a family member remind them that they practiced straightening for years.
Langerhans Cells in LPP and Traction Alopecia
A study comparing the Langerhans cell concentration in LPP with traction alopecia was performed using double immunostaining with CD1a and CD3. The 16 biopsy specimens evaluated included nine biopsies of LPP and seven biopsies of traction alopecia. The mean ratio of the concentration of Langerhans cells to T lymphocytes was 1.28 for LPP and 0.59 for traction alopecia, suggesting the inflammation in LPP may be influenced by Langerhans cells and suggesting that traction alopecia is not immune-mediated. It should be noted that isolated cases of traction alopecia demonstrated ratios similar to those seen in LPP, limiting the diagnostic utility in individual cases. It may be that these cases represented cicatricial marginal alopecia, rather than traction alopecia.
Elastic Tissue Patterns in Alopecia
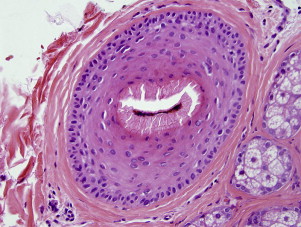
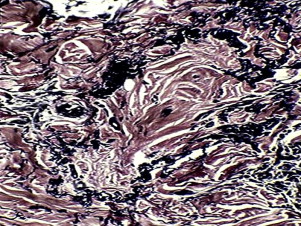
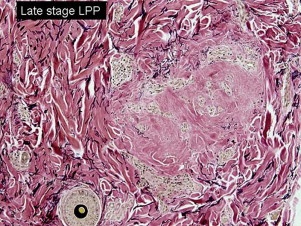
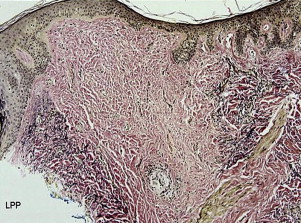
Characteristic patterns of elastic tissue loss can be helpful in the diagnosis of scarring alopecia. The biopsy must be taken from a mature area of alopecia and does not require the presence of inflammation. Normal fibrous tract remnants are surrounded by a thick elastic tissue sheath ( Fig. 6 ). LPP and folliculitis decalvans demonstrate loss of the elastic sheath in the late stage when the infiltrate is no longer identifiable ( Fig. 7 ). In vertical sections, LPP and folliculitis decalvans demonstrate superficial wedge-shaped scars centered about the infundibulum ( Fig. 8 ), whereas end-stage lesions of chronic cutaneous lupus erythematosus usually demonstrate loss of elastic tissue throughout the entire dermis. Idiopathic pseudopelade (ie, those cases that do not represent LPP) demonstrates broad hyalinized fibrous tract remnants with preservation and duplication of the elastic sheath and thick interstitial elastic fibers ( Fig. 9 ). Although an elastic van Gieson stain is most commonly used to demonstrate the characteristic patterns, an alternative is to view hematoxylin-eosin stained sections under a fluorescent microscope, taking advantage of the autofluorescence of the eosinophilic elastic fibers ( Fig. 10 ). This compares favorably with elastic van Gieson stained sections ( Fig. 11 ). It should be emphasized that elastic staining provides prognostic and diagnostic information, because scarring at the level of the germinative epithelium (bulge area) correlates with permanent hair loss.
Related posts:
 Cytogenetic and Mutational Analyses of Melanocytic Tumors
Cytogenetic and Mutational Analyses of Melanocytic Tumors
 Dermatology Clinics
Fibrous and Fibrohistiocytic Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Dermatology Clinics
Fibrous and Fibrohistiocytic Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


