Abstract
The advent of computer-aided design and manufacturing (CAD/CAM) and virtual surgical planning (VSP) has resulted in a transformation in our approach to primary and secondary reconstruction of craniofacial trauma. Ever more complex defects are able to be securely addressed with innovative preoperatively planned solutions. The ability to visualize both the problem and operative solution in a virtual forum and plan each step prior to entering the operating room means that potential challenges can be addressed in advance and the operative approach refined accordingly. Moreover, the creation of anatomically personalized implants using 3D printing techniques in combination with VSP means that a more exact and predictable outcome can be achieved. These tools intuitively lend themselves to the most complex of trauma cases. The field is constantly evolving, with exciting novel applications on the horizon. These include coupling of bioactive substances such as growth factors and cells with custom implants. Thus, we expect VSP to become increasingly useful in combination with these innovations in achieving a more natural result in reconstructive surgery.
Keywords
virtual surgical planning, CAD/CAM, 3D printing, orbital reconstruction, mandible reconstruction, midface reconstruction
Background
Since its emergence in the late 1980s, computer-assisted surgery (CAS) has become an increasingly important adjunct to craniofacial reconstruction. The refinement of virtual surgical planning (VSP) coupled with the availability of 3-dimensional (3D) printing techniques has enabled easier and more predictable remodeling of the craniofacial skeleton. As these techniques continue to develop, they point to a future in which ever more elaborate craniofacial challenges can be tackled with more secure outcomes. In this chapter we discuss the utility of CAS techniques for primary and secondary trauma reconstruction and then consider the future of these approaches in craniofacial surgery.
The groundwork for contemporary CAS was established in the 1980s with the proliferation of CT scanning and the advent of computer-aided design and manufacturing (CAD/CAM) methods. By enabling noninvasive, 3-dimensional visualization of the craniofacial skeleton, the former enabled much more accurate preoperative diagnosis and planning than was available from plain radiographs. Utilization of CAD/CAM in turn allowed that preoperative plan to be translated into adjuncts for surgery such as patient-specific cutting guides and implants. The integration of these techniques into a unified computer-assisted craniofacial surgery was first described by Toth et al. in 1988. These authors generated patient-specific resin molds which were then used preoperatively to shape prosthetic implants and intraoperatively to guide bone shaping in a series of patients needing frontoorbital reconstruction. The subsequent revolution in digital image manipulation allowed this pioneering approach to be much more widely adopted.
Contemporary Uses of CAS
Currently CAS techniques are commonly used in elective craniofacial and orthognathic surgery as well as in craniofacial trauma reconstruction. The utility of these approaches has been widely chronicled in the literature. Some of the broad categories of applications include VSP of osteotomies, segmental bone movements or reductions, virtual correction of occlusion, generation of customized cutting guides, and creation of patient-specific implants. These applications largely share a common workflow: (1) acquisition of high resolution CT images of the craniofacial skeleton; (2) conversion of these images to DICOM file format for use in digital image manipulation; (3) creation of 3D reconstructions of the craniofacial skeleton by a bioengineering company; (4) VSP teleconference between surgeons and biomedical engineers to discuss surgical plans; (5) creation of patient-specific implants, models, or cutting guides. Completion of this workflow can be accomplished in a week or less and has been shown to be cost-effective when considering its acceleration of operative times. We next illustrate the use of CAS in primary and secondary trauma reconstruction.
Primary Reconstruction
Utilization of CAS in primary craniofacial trauma reconstruction presents some challenges. The time required to complete CAS workflow may limit its utilization, though this process is becoming ever more expeditious. In general we advocate early treatment of facial fractures in order to achieve the most anatomic repairs and to minimize unfavorable scarring and soft tissue contraction. However, in the severely injured trauma patient, where CAS techniques are most useful, there is often time between initial stabilization of injuries to other body systems and definitive repair of craniofacial injuries. Advantages of CAS in these situations include minimization of dissection and more accurate repairs through the use of pre-bent plates and cutting guides. These benefits are particularly valuable in severe craniofacial injuries in which multilevel trauma and comminution can disrupt normal anatomic relationships that guide repair. We present an example in which CAS proved valuable in reconstruction of the mandible.
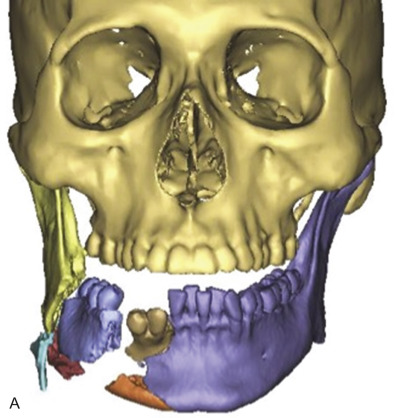
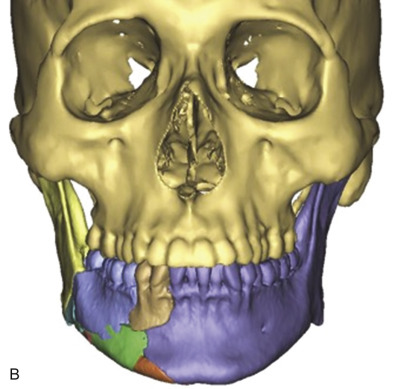
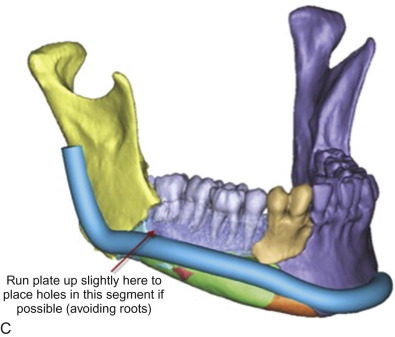
We used CAS techniques to virtually reduce a severely comminuted mandible fracture following a blast injury ( Fig. 3.14.1 ). The patient was involved in a chemical explosion at work and suffered injuries to his lower face including degloving of skin and soft tissues of the right cheek and open fractures of the right mandibular body and parasymphyseal region with significant comminution. After primary stabilization and placement of a tracheostomy at the regional burn center, the patient was transferred to our care for management of his facial injuries. The numerous fragments of mandibular bone – some of marginal viability – made accurate anatomical reduction challenging. Proper reduction and fixation was further complicated by the need to minimize additional soft tissue dissection for fear of compromising blood supply to the bone. For these reasons, we conducted a VSP planning session in which major fragments were brought into alignment virtually. Additionally, proper occlusion was established in this forum and used to guide design of a pre-bent reconstruction plate spanning the aligned fragments. This plate was milled and shipped to our center in 5 days. Intraoperatively, the patient’s existing traumatic lacerations were extended and conservative debridement of clearly nonviable soft tissue and bone was performed. After simplification of smaller fracture fragments through a combination of bridle wiring and 1 mm superior border plates, the patient was placed in maxillomandibular fixation using Erich arch bars and elastics. These were secured to major fracture fragments with bone reduction forceps and digital manipulation. The custom plate was then readily adapted to the reduced mandible and secured using locking screws. The patient has gone on to heal with restoration of premorbid occlusion at his most recent 2-month follow-up.


Secondary Reconstruction
The improved preoperative diagnosis and planning afforded by VSP is particularly useful in complex secondary reconstructions. These cases are challenging due to anatomic distortions and scarring caused by primary surgery, the requirement for debridement or corrective osteotomies, and the effacement of bony landmarks due to malunion or nonunion. In these cases the craniofacial surgeon must often remove what was suboptimal from the original surgery before crafting a de novo patient-specific solution. We describe some examples in which these principles are utilized to effect secondary repair of the mandible and orbit.
Mandible
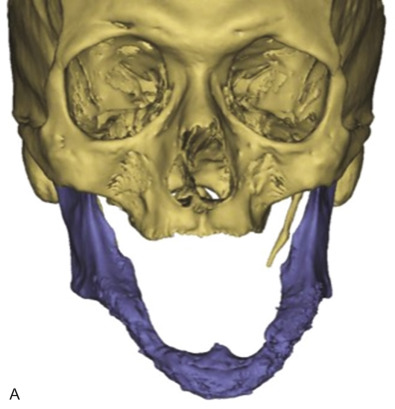
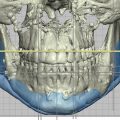
We have used VSP to correct malunion of an edentulous mandible ( Fig. 3.14.2 ). Accurate repair of mandible fractures in edentulous patients is challenging, as the lack of occlusal guidance makes accurate reduction difficult and poor bone stock complicates fracture healing. In this example, the patient was a 69-year-old man who sustained bilateral body fractures after a fall 7 months prior to our repair. He originally underwent open reduction and internal fixation with miniplates, but this was complicated by plate failure. A revisional surgery was performed with hardware removal and reconstruction using a single load-bearing reconstruction bar spanning both fractures. This repair was complicated by malunion, however. Therefore, on presentation to our institution, the patient had an anterior open-bite with inability to masticate. As the patient was edentulous in both mandible and maxilla, VSP was instituted to place the mandible in a more functional position. Prefabricated cutting guides were generated to ensure accurate realignment of the malunited mandible and a pre-bent reconstruction plate was obtained to secure the osteotomized segments. Using these adjuncts repair was performed expeditiously. The patient achieved anatomic union and was able to masticate with the aid of dentures at a 6-month follow-up.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


