Introduction
In order to understand treatment of various venous disorders, it is necessary to know the normal anatomy and function of the venous system of the lower extremities so as to better understand deviations from normality.
Nomenclature is particularly important since it is difficult to discuss the topic of leg veins without agreement about definitions and meaning. In 2001, an International Interdisciplinary Committee was designated by the Presidents of the International Union of Phlebology (IUP) and the International Federation of Anatomical Associations (IFAA) to update the official Terminologia Anatomica regarding the veins of the lower limbs. Deficiencies in the previous official Terminologia Anatomica had resulted in nonuniform anatomical nomenclature in the clinical literature that complicated international exchange of information and possibly resulted in inappropriate treatment of venous disease. The Committee, with the participation of Members of the Federative International Committee for Anatomical Nomenclature (FICAT), developed a Consensus Document at a meeting held in Rome on the occasion of the 14th World Congress of the IUP. The recommendations of the Committee were published in 2002 ( ).
The Committee refined and extended the proposed terminology in 2004 during the 21st World Congress of the International Union of Angiology (IUA), under the auspices of the IUP, IFAA and FICAT. Nomenclature of the deep and perforating veins was not criticized. The revised document primarily addressed new terms and the nomenclature of the pelvic and superficial leg veins. A summary of important changes in nomenclature of the lower extremity veins are listed in Table 1.1 . These new, occasionally unfamiliar terms are used in the following exposition.
| Old terminology | New terminology |
|---|---|
| Femoral vein | Common femoral vein |
| Superficial femoral vein | Femoral vein |
| Deep vein of the thigh | Profunda femoris vein |
| Sural veins | Soleal veins, gastrocnemius veins (medial and lateral) |
| Greater or long saphensous vein | Great saphenous vein (GSV) |
| Smaller or short saphenous vein | Small saphenous vein (SSV) |
| Giacomini’s vein | Intersaphenous vein |
| Huntarian perforator | Mid-thigh perforator |
| Boyd’s perforators | Paratibial perforators |
| Dodd’s perforator | Perforator of the femoral canal |
| Cockett’s perforators | Posterior tibial perforators |
| May’s perforator | Ankle perforators |
| Sherman’s perforator | Paratibial perforator |
| Gastrocnemius point | Intergemellar perforator |
Anatomy
The venous system in the lower extremities can be divided, for purposes of understanding, into three systems: the deep system, which parallels the tibia and femur; the superficial venous system, which resides in the superficial tissue compartment between the deep muscular fascia and the skin; and the perforating or connecting veins, which join the superficial to the deep systems. The perforating veins are thus named because they penetrate anatomical barriers.
Although the superficial veins are the targets of most therapies, the primary return of blood flow from the lower extremities is through the deep veins. In the calf, these deep veins are paired with and named for their accompanying arteries. Specifically, the anterior tibial, posterior tibial, and peroneal arteries are accompanied by their paired veins, to which they are interconnected. These crural veins join to form the popliteal vein. Occasionally the popliteal vein and femoral vein are paired like the calf veins.
As the popliteal vein ascends, it becomes the femoral vein, formerly called the superficial femoral vein. Near the groin, the femoral vein joins the deep femoral vein, and the two become the common femoral vein, which ascends to become the external iliac vein proximal to the inguinal ligament.
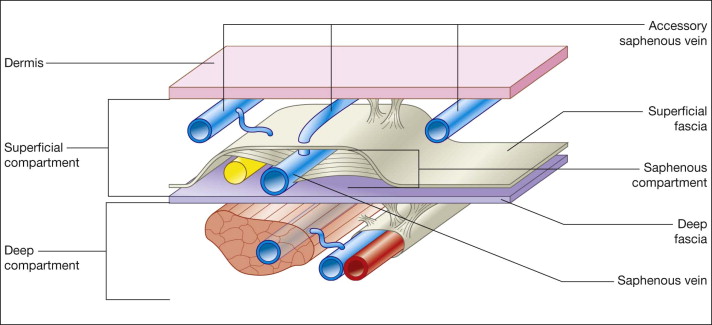
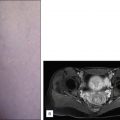
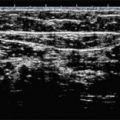
Ultrasound imaging has shown that the superficial compartment of the lower extremity is in fact comprised of two compartments, one enclosing all of the structures between the muscular fascia and the skin. The other is within the superficial compartment and encloses the saphenous vein. It is bounded by the muscular fascia inferiorly and the superficial fascia superiorly. It is termed the ‘saphenous compartment’ ( Fig. 1.1 ). The importance of this anatomic structure, the saphenous compartment, is underscored by its being targeted during percutaneous placement of endovenous catheters and the instillation of tumescent anesthesia.
The main superficial veins are the great saphenous vein (GSV) and small saphenous vein (SSV). Each of these has many interconnecting tributaries, referred to as communicating veins. The GSV originates on the dorsum of the foot, from where it ascends anterior to the medial malleolus of the ankle and further onto the anteromedial aspect of the tibia. At the knee, the GSV is found in the medial aspect of the popliteal space. It then ascends through the anteromedial thigh to join the common femoral vein just below the inguinal ligament. Throughout its course, it lies within the saphenous compartment.
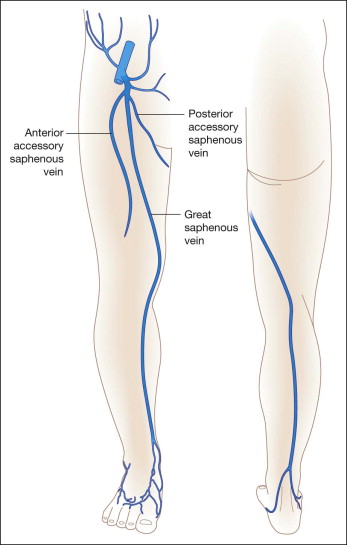
Other venous segments may also be found within the fascial compartment in the thigh, parallel to the GSV. Such venous segments are identified as the anterior or posterior accessory saphenous veins depending on their anatomical location in respect to the GSV ( Fig. 1.2 ). Real anatomic doubling of a vein occurs only when the two veins show the same path, topography and relationships, such as the tibial or peroneal veins.
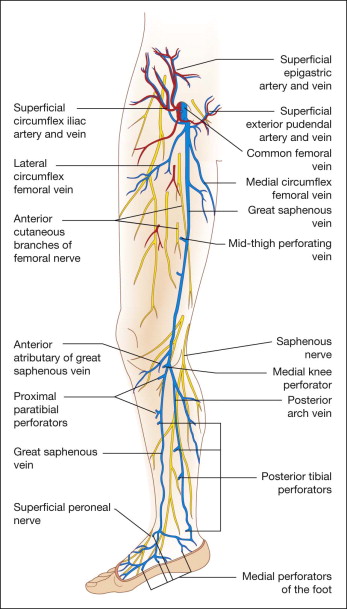
The SSV originates laterally from the dorsal venous arch of the foot and travels subcutaneously behind the lateral malleolus at the ankle. As it ascends in the calf, it enters the deep fascia and courses between the heads of the gastrocnemius muscle to join the popliteal vein behind the knee ( Fig. 1.3 ). The SSV usually empties in to the popliteal vein directly or via the gastrocnemius vein but there are many anatomic variations in its points of connection to the popliteal vein. The cranial extension of the SSV may be present and is a tributary that continues in the cephalad direction. Rarely, the SSV may empty into the femoral vein or join the GSV directly, without emptying into the popliteal vein. In as many as one third of patients, the cranial extension of the SSV drains into a posterior medial tributary of the GSV or directly into the GSV via the intersaphenous vein, or into a deep vein in the thigh via a perforator.
The intersaphenous vein is a communicating vein that connects the SSV to the GSV in the posterior-medial aspect of the leg. This vein courses the posterior thigh as a tributary or extension of the SSV and has many variations in its termination. The intersaphenous vein is also known as the vein of Giacomini, named after the Italian Professor of Anatomy who orignially described it in 1873. Although the use of eponyms in venous nomenclature is generally discouraged, the vein of Giacomini is one of the few acceptable terms bearing the name of its founder ( Table 1.2 ). Table 1.3 summarizes common anatomical terms used to describe the superficial veins of the leg.
| Giacomini’s vein | Designates the medial thigh anastomosis between the SSV with the GSV. Giacomini’s vein corresponds to the posterior thigh circumflex vein, which may originate from the SSV or from its thigh extension, and ends in the GSV or its posterior accessory |
| Posterior arch vein | Designates the vein that lies on the medial surface of the leg, posterior and parallel to the GSV. It corresponds to the leg portion of the posterior accessory of the GSV |
| Cockett’s perforating veins | Correspond to the posterior tibial perforators that connect the posterior arch vein with the posterior tibial veins |
| Santorini’s plexus | This term, commonly used by urologists, is used to describe the retropubic vesico-prostatic plexus |
| Anatomical term | Description |
|---|---|
| Great saphenous vein (GSV) | The GSV runs along the medial malleolus and ascends through the anteromedial calf and thigh to join the common femoral vein just below the inguinal ligament. It is bound by the saphenous compartment |
| Sapheno-femoral junction (SFJ) | The SFJ is the term used to describe the point at which the saphenous vein terminates proximally at the inguinal ligament and meets the femoral vein |
| Superficial circumflex iliac vein | A vein that corresponds to the superficial circumflex iliac artery and empties usually into the great saphenous vein |
| Anterior accessory of the great saphenous vein (AASV) | The AASV runs in the thigh anteriorly with respect to the GSV, but has its own saphenous compartment |
| Posterior accessory of the great saphenous vein, or Posterior accessory saphenous vein (PASV) | The presence of a PASV is less common than the AASV. It is in the thigh located posteriorly with respect to the GSV, but has its own saphenous compartment |
| Small saphenous vein (SSV) | The SSV runs along the lateral malleolus and ascends via the posterior calf to join the popliteal vein behind the knee in the popliteal fossa |
| Sapheno-popliteal junction (SPJ) | The SPJ is the termination of the SSV with the popliteal vein. This most often lies 2–4 cm above the popliteal skin crease but its exact location is variable |
| Cranial extension of the small saphenous vein | The cranial extension of the small saphenous vein courses in the groove between the biceps femoris and semimembranosus muscles. This vein has been called ‘femoropopliteal vein’ |
| Anterior thigh circumflex vein | A tributary of the GSV or AASV that ascends obliquely in the anterior thigh. It may originate from the lateral venous system |
| Posterior thigh circumflex vein | A tributary of the GSV or PASV which ascends obliquely in the posterior thigh. It may originate in the SSV, its thigh extension, or the lateral venous system |
| Tributary veins | Tributaries are branches of the GSV or SSV that lie outside the saphenous compartment |
| Intersaphenous veins | Intersaphenous veins connect within the same anatomic layer in contrast to perforating veins, which break through fasica to connect the superficial to deep veins. The intersaphenous vein that runs obliquely in the leg to connect the SSV and GSV is known as the vein of Giacomini |
| Lateral venous system | The lateral venous system is extended on the lateral thigh and leg. It represents the remnant of the embryonic vena marginalis lateralis |
| Dorsal venous arch of the foot | The dorsal venous arch gives rise to two or three veins of the dorsum of the foot, which sometimes merge to join the great saphenous vein or to form an accessory saphenous vein |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


