“Losses must be replaced in kind.” Sir Harold Gillies
Historical Background
Advances in regenerative medicine have opened a new era and enabled reconstruction of devastating soft and bony tissue defects due to trauma, congenital deformities, and neoplastic conditions. Among the most promising advances within the realm of regenerative and restorative surgery is vascularized composite allotransplantation (VCA), which now allows for the reconstruction of defects that previously would have been treated with multistage flap reconstructions or prostheses. Similar to solid organ transplant (SOT), VCA involves transplantation of a vascularized graft, which is derived from different embryogenic origins and composed of a variety of heterogeneous antigenic tissues, across a genetic mismatch.
Replacement of lost limbs and other organs is an old desire of humanity. The first historical mention of VCA dates back to Saints Cosmas and Damian (AD 286), who transferred an Ethiopian Moor’s limb to a churchman. Later, successful solid organ transplantations constituted the initial milestones of VCA. The first successful human allograft was performed in 1957 by E. Peacock. The allograft was composed of an en bloc digital flexor tendon mechanism. However, this transplantation did not contain skin. In the 1960s, immunosuppression was limited, which lead to the unfortunate rejection of the world’s first hand transplant attempted by Robert Gilbert in 1964. Two weeks after the surgery, the graft was explanted and re-amputation was performed. This complication delayed the next clinical hand transplantation, but studies about immunosuppression and experimental models continued to evolve to solve the problem. Once the clinical efficacy of cyclosporine (CsA) had been demonstrated in solid organ transplantation, studies were begun performing limb allograft transplantation in rats, dogs, and rabbits. In 1985, Hewitt reported the first successful rat limb allotransplantation. He also showed that transplanted bone marrow was functional and caused immune chimerism. During the same time period, Achauer mentioned the potential use of allografts for facial reconstruction. The first successful face transplantation in rats was performed by Maria Siemionow and colleagues. Subsequently, many models of VCA were developed and reported in both small and large animals. , Pharmacological research continued during this time and new drugs were developed for immunosuppression. In 2003, Siemionow reported the first and the only rat transplant model of life-long donor-specific tolerance using a 7-day protocol of anti-alphabeta T-cell receptor monoclonal antibody and CsA.
During the past 50 years, various clinical and experimental composite tissue allotransplantations have been performed, including: limb, trachea, flexor tendon apparatus, penis, nerve, knee, hand, face, abdominal wall, and uterus. ,
Nomenclature
Autograft is a tissue that is transplanted from one location to another in the same individual. When the graft is transplanted from a genetically identical donor, such as transplants between syngeneic animals and human monozygotic twins, it is called isograft . Allograft is transplantation of tissues between genetically different individuals of the same species whereas xenograft is transplantation between different species.
Transplantation may also be described in terms of the site where the tissue is transplanted. Orthotopic transplantation means the recipient site is an anatomically similar site and heterotopic transplantation means the recipient site is different from the site of origin. In clinical practice, human kidney transplantation is performed to the groin region of the recipient, which is a heterotopic transplantation.
Despite the encouraging results, debate continues over the immunosuppression-related risks. Thus, the ultimate goal of allotransplantation is to obtain transplant tolerance , which is rejection-free acceptance of transplanted organs or tissues without the need for long-term immunosuppression. Donor-specific tolerance is defined as the state of donor-specific hyporesponsiveness in the recipient of allograft in the absence of immunosuppression. The state of tolerance to one organ or tissue (such as tendon) while simultaneously rejecting another (such as skin) is called split tolerance . One of the best approaches to obtaining tolerance is hematopoietic stem cell chimerism. In chimerism , tissues from two genetically different organisms coexist in one organism. There are two types of chimerism: macrochimerism occurs when bone marrow is transplanted to a conditioned recipient, is engrafted, and produces all cell lineages; microchimerism arises from the migration of donor leucocytes from the allograft to the recipient and in microchimerism donor hematopoietic stem cells do not engraft, but are produced and migrated systemically.
Basic Transplantation Immunology
Rejection is the major barrier to successful transplantation. During the immune response several interactions between the innate and adaptive immune system will lead to the rejection of transplanted cells, tissues, or organs unless the immune response is suppressed. The most important antigens contributing to allograft rejection are the major histocompatibility complex (MHC) antigens. The MHC proteins are encoded in chromosomes and have different nomenclature between species: human lymphocyte antigen (HLA) in humans, swine lymphocyte antigen (SLA) in swine, and RT1 in rat. There are two major classes of major histocompatibility complex (MHC) antigens. Class I antigens are expressed on nearly all nucleated cells and serve as the primary target for cytotoxic (CD8 + ) T lymphocytes. Class II antigens are expressed primarily on vascular endothelium, antigen-presenting cells (APC), B cells, and activated T cells. Both class I and class II molecules have a specific site at which foreign peptide antigens can be presented after they have been processed by the cell. Innate immune system is activated as a result of ischemia–reperfusion injury, surgery, and trauma. Following this activation, foreign antigens are recognized by host T cells after being processed by host antigen-presenting cells (APC). This is called indirect presentation . In addition, host cells can recognize donor MHC antigens, which is called direct presentation .
The allograft rejection or allorecognition is primarily regulated by T lymphocytes. The T cell lineage marker is called T-cell receptor (TCR) and there are two different types of T cells: alphabeta T cells, which are responsible for the allograft rejection, and gammadelta T cells, which are responsible for infections and antitumor activity. Mature alphabeta T cells are subdivided into two groups. T helper cells induce immune response and are CD4 positive. Cytotoxic T cells are responsible for cytotoxicity and are CD8 positive. Following allotransplantation, rejection begins with activation of T cells and T cells require a minimum of two signals for activation. The first step of T cell activation is recognition of foreign antigen by T cells (signal 1). The second step is activation of co-stimulatory signals (signal 2). The third step is T cell differentiation, which involves recreation of interleukin-2 following co-stimulatory signals (signal 3). Activated T cells are responsible for cell-mediated rejection of the allograft. ,
Different types of allograft rejection may occur and are regulated by different mechanisms. Hyperacute rejection occurs within a few minutes after transplantation. This immune response is an antibody-mediated rejection process and the most frequent reason is the presence of pre-sensitized antibodies against MHC antigens. Acute allograft rejection is a cell-mediated immune response and is observed in almost all composite tissue allotransplantation cases. The incidence of acute rejection exceeds 80% in hand and face transplants. It is primarily attributed to T cell activation. There is not enough data about antibody-mediated rejection (AMR) in VCA, although vascular rejection in solid organs is attributed to AMR. Although not seen in the rat limb transplant model, there are several clinical case reports showing a B-cell-driven rejection episode with presence of donor-specific antibodies (DSA) and C4d positivity. However, it remains unclear whether these rejections were “truly” antibody-mediated or whether antibodies were bystanders of the rejection process.
Chronic rejection is a common characteristic of solid organ transplantation; however, there are currently insufficient data available to define specific changes of chronic rejection in the VCA. The overall incidence of chronic allograft rejection in VCA recipients is low but has to be put in the context of the relatively short follow-up periods for most of the VCA transplants. Chronic rejection is characterized by fibrotic changes, myointimal proliferation of arteries and arterioles, loss of adnexa, skin, and muscular atrophy, and fibrosis of deep tissues, which may be caused by non-immunogenic factors such as ischemia. Thus, the mechanisms of chronic rejection and its significance in VCA survival need further investigation.
In order to define and classify VCA rejection, various classification systems have been developed. The most accepted system for VCA rejection is the Banff 2007 Working Classification. There are four grades of rejection: grade I mild, grade II moderate, grade III severe, and grade IV necrotizing acute rejection. In this system, the defining features to diagnose acute skin rejection include: inflammatory cell infiltration with involvement of epidermis and/or adnexal structures, epithelial apoptosis, dyskeratosis, and necrosis. This classification system is accepted by the International Society for Vascularized Composite Allotransplantation. Although, AMR and chronic rejection have not been implemented into the Banff 2007 classification, the Banff 2013 Meeting reported: “Current observations are that chronic VCA rejection is more similar than different from that in other organ transplants.” The Banff 2013 Meeting Committee agreed to collect data for potential changes to the VCA–Banff system.
Transplant immunology is the most important research area in the VCA field and many current studies attempt to define our knowledge and understanding of the rejection mechanisms, routine immunosuppressive regimes and tolerance-inducing strategies. Today, the only method of allograft rejection prevention is administration of chronic immunosuppression. There are several new drugs and protocols, which are used experimentally and clinically. However, the ultimate goal of transplant immunology is to provide donor-specific tolerance.
The practice of immunosuppressive administration can currently be divided into three phases: induction, maintenance, and rescue therapies. Induction immunotherapy is used as a means to overcome the ischemia–reperfusion injury and surgical trauma an allograft undergoes during the transplant procedure. Maintenance therapy is defined as immune suppression that is typically much lower in dose than induction therapy and therefore applicable in a chronic setting. Rescue therapy is similar to induction therapy in that it employs high-dose immune suppression and is usually given in response to a rejection episode. The efficacy of local immunosuppression in clinical VCA remains controversial. Topical treatments with steroid and tacrolimus ointments have achieved sufficient resolution of low-grade rejections. Immunosuppressive therapy has well-documented side effects which may give rise to conditions that shorten life. The incidence and severity of such side effects are well described, and this would allow for an informed decision to be made as to whether these side effects outweigh the potential benefit from VCA.
Experimental Models of VCA Transplantation
Experimental animal models constitute the workhorse of the VCA as they help to determine the technical feasibility and evaluate the effects of various immunosuppressive protocols and novel tolerance-inducing strategies.
Animal Models
During the past 20 years, many VCA models were developed to test the feasibility of transplantation of different body components as well as to assess the effects of various immunosuppressive protocols. The experimental models can be divided into two main categories, namely small and large animal models, including nonhuman primate models. Another classification of experimental models is based on the type and the content of the transplanted allograft:
- •
skin-containing VCA models (groin flap, abdominal wall, etc.)
- •
composite hindlimb allograft transplantation models (limb, groin–thigh osteomyocutaneous flap, knee allograft)
- •
composite facial allograft transplantation models (full face, hemiface, midface etc.)
- •
immunomodulatory VCA models (vascularized bone marrow, femur, sternum thymus).
The basic experimental models and their specific features are summarized in Table 11.1 .
| Experimental Model | Tissues Included, Specific Features |
|---|---|
| Skin-containing VCA Models | |
| Groin flap as vascularized skin transplant model | Skin, fat, and lymphoid tissue. Simple, used in immunologic studies, small skin component |
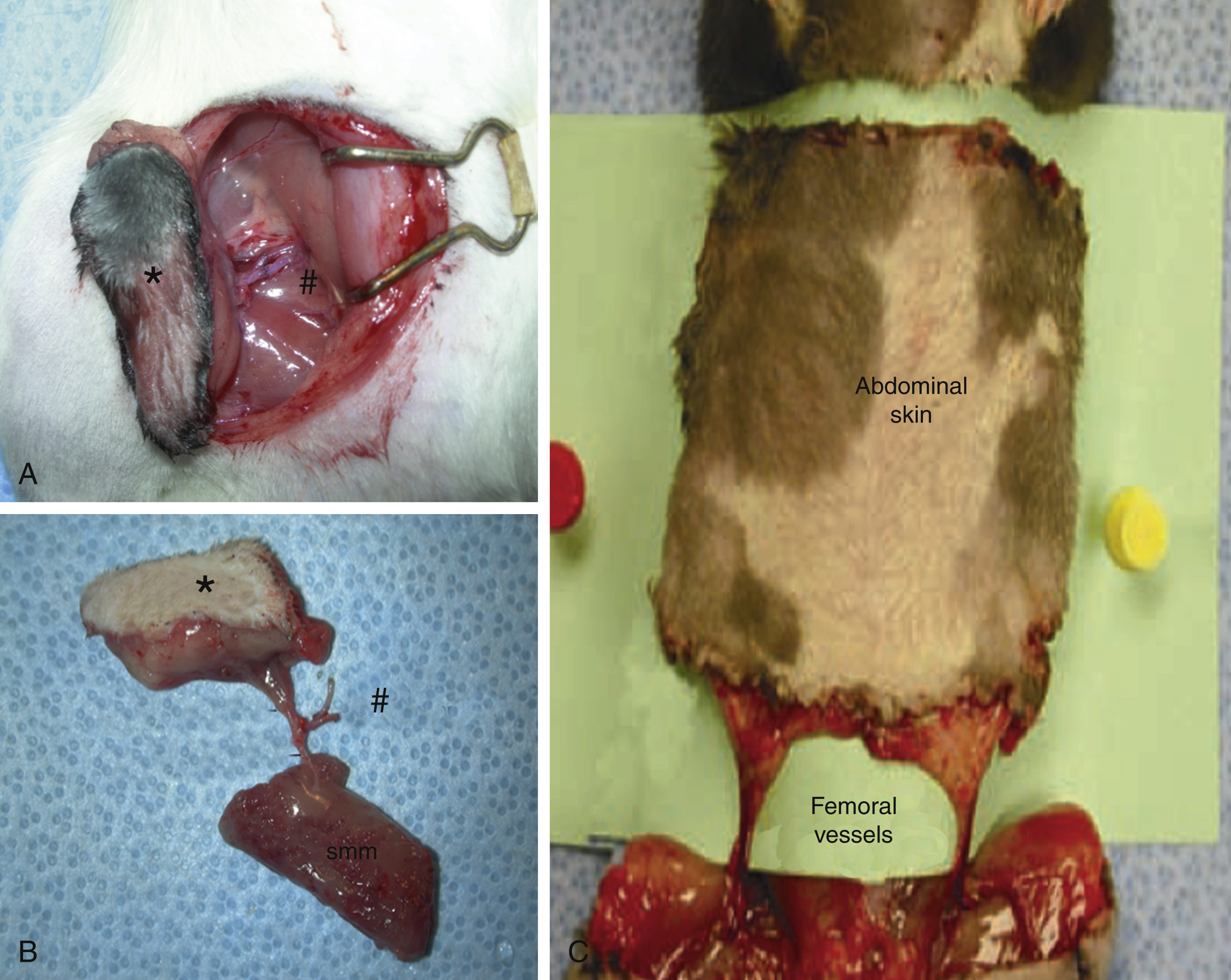
| Semimembranosus muscle and epigastric skin transplant model | Skin, fat, muscle, and lymphoid tissue. Used for microcirculatory, physiologic, and immunologic studies |
| Total abdominal wall transplant model | Skin, fat, and lymphoid tissue. Contains large skin component |
| Hindlimb Models | |
| Rat hindlimb transplant model | Popular, but technically challenging animal model containing all tissue components including vascularized bone marrow |
| Groin–thigh osteomyocutaneous transplant model | Alternative model to hindlimb transplant. Less challenging technique, low mortality |
| Immunomodulatory VCA Models | |
| Vascularized femur transplant model | Femoral bone, bone marrow, cartilage and muscle. Applied for bone marrow induced chimerism studies |
| Bilateral vascularized femoral bone transplant model | Larger bone marrow content. Applied for tolerance induction studies |
| Composite vascularized skin/bone transplant model | Combination of groin flap with vascularized femur transplantation. Enables follow-up of rejection |
| Vascularized osteomyocutaneous iliac transplant model | Iliac bone, bone marrow, abdominal wall musculature, and wide skin island |
| Vascularized sternum transplant model | Sternum, skin, and muscles. Contains bone marrow |
| Thymus transplant model | Used for evaluation of effect of thymus on tolerance induction |
| Osteomyocutaneous sternum, ribs, thymus, pectoralis muscles, and skin transplant | Includes all three important immunological tissues (bone marrow, thymus, and skin) for immunology and tolerance studies |
| Facial Allograft Models | |
| Full face/scalp transplant model | Includes ear, neck, and facial skin without eyelids and nose. High mortality |
| Hemiface/scalp transplant model | Unilateral ear, neck, and facial skin. Used for immunological studies in facial transplantation |
| Hemiface calvarium transplant model | Temporal muscle and parietal bone included to hemiface scalp model. Contains bone marrow |
| Hemiface mandible tongue allotransplantation model | Mandibular bone and tongue are included into hemiface model. Contains bone marrow |
| Maxilla transplant model | Evaluation of response of maxillary bone to transplantation |
| Midface transplant model with sensory and motor units | First model to evaluate motor and sensory recovery after face transplantation |
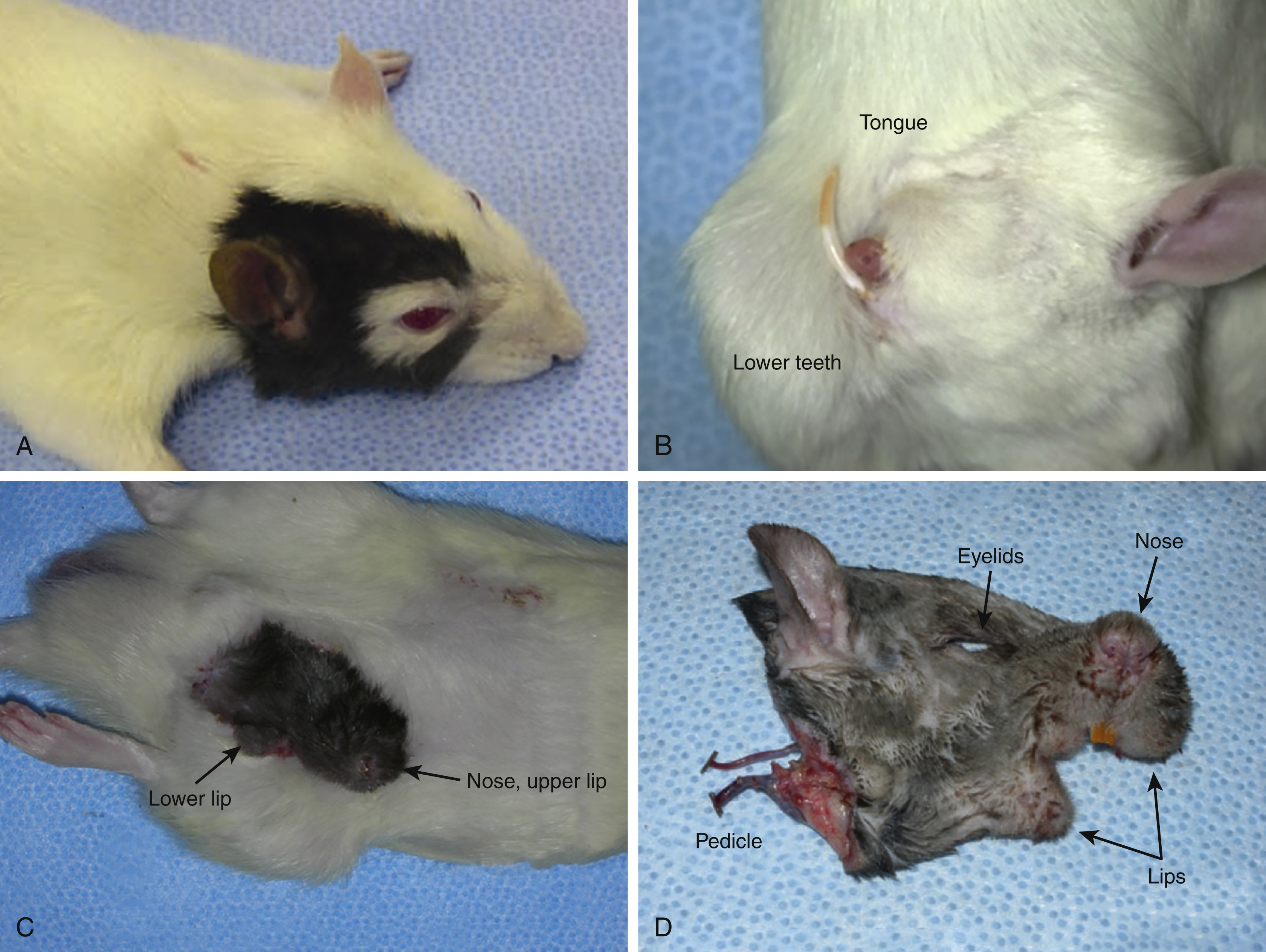
| Total osteocutaneous hemiface transplant model | Includes entire hemiface: vascularized nose, premaxilla, eyelids, upper and lower lips, external ear and facial skin for immunological, histological, and biological evaluation of different facial tissues |
| Composite face and eyeball transplant model | Evaluation of optic nerve regeneration and evaluation of orbit content |
Skin and Soft Tissue VCA Models
These models include allografts containing skin, subcutaneous tissue, fat, and muscle ( Fig. 11.1 ). The most frequently used skin-containing VCA model is the groin flap. This flap is also one of the first models used in allotransplantation research. The groin flap model contains skin, fat, and lymphoid tissue harvested on the superficial epigastric vessels or femoral vessels. The groin flap is frequently used in immunological studies as it is technically simple and has low mortality. However, a disadvantage stems from the small size of the skin paddle. Other soft tissue flaps include both skin and various muscles, such as the semimembranous pectoralis flaps. Another soft tissue model is the total abdominal wall transplantation in which the entire abdominal wall skin is harvested on bilateral femoral vessels. This model was developed to investigate the effect of size of skin component on the development of chimerism. Fig. 11.1 presents examples of the skin and soft tissue models of VCA.
Hindlimb Allotransplantation Models
The rat hindlimb transplantation model was described in 1978. In this model a circumferential skin incision at the mid-thigh level is made on the donor and next the superficial epigastric vessels, femoral vessels, saphenous nerve, and femoral nerve are dissected, and thigh muscles are sharply divided. During muscle transection, the sciatic nerve is dissected. Next, the femoral bone is cut with a saw. The recipient is prepared using the same technique. Following division of the donor femoral vessels the limb is transferred to the recipient. First, the femoral bone is fixed with an intramedullary rod and wire suture. The femoral vessels are subsequently anastomosed and the femoral, sciatic, and saphenous nerves are coaptated. Muscles and skin are closed anatomically. Hindlimb transplantation in the rat is a complex procedure involving connection of bone, muscles, nerves, vessels, and skin. The rat hindlimb allograft transplant is the most popular animal model tested in preparation for human hand transplantation. This underlies the importance of having a fast, simple surgical procedure (with short anesthesia) that provides good animal recovery and consequently robust data for statistical assessment. In order to obtain a fast and simple limb allotransplantation method, Chang et al described a groin–thigh osteomyocutaneous flap, which is composed of skin (groin), muscle (thigh), and bone (⅔ femur), based on the femoral vessels and superficial epigastric vessels. The advantages of this model are shortened operative time, easy monitoring of graft rejection, decreased morbidity and mortality rates, and earlier postoperative ambulation.
Facial Allograft Transplantation Models
Since the face has many different anatomical structures and units, there are many facial allograft transplantation models, developed to evaluate transplantation of different facial structures ( Fig. 11.2 ). Siemionow et al were the first to develop a full-face scalp allotransplantation model. This facial allograft transplant, which includes bilateral ear, neck, and facial skin without eyelid and nose skin, is based on the bilateral common carotid artery and external jugular vein. However, the surgical procedure of full-face transplantation was challenging, with a high rate of mortality. Thus, a hemiface scalp allotransplantation model was developed in the Cleveland Clinic Laboratories. This model included the unilateral scalp, ear, neck, and facial skin – excluding eyelid and nose – and was based on the unilateral common carotid artery and external jugular vein. The hemiface scalp allotransplantation model is generally used for immunological studies assessing facial allograft transplantation. Yazici et al developed a hemiface calvaria model by including temporal muscle and parietal bone to the prior hemiface scalp model. This model included parietal bone, with bone marrow cells, which were viable up to 100 days post transplant as confirmed by histology. The facial allograft model, containing mandible with bone marrow cells, was later described by Kulahci et al. In this heterotopic allotransplantation model including hemiface mandible and tongue, Kulahci et al showed high levels of donor-specific chimerism. In the maxilla allotransplantation model, the maxilla was dissected along Le Fort II osteotomy lines based on the common carotid artery and external jugular vein and the harvested allograft was transplanted to the recipient. This model was developed to evaluate the maxillary response to allotransplantation. The first model that evaluated the motor and sensory recovery after facial allotransplantation was developed by Zor et al. This composite midface transplant model with the sensory and motor neuromuscular units included premaxilla, mystacial pad, and nose with infraorbital and facial nerves. At 100 days post transplant, somatosensory evoked potentials (SSEP) and motor evoked potentials (MEP) tests revealed that sensory and motor recovery reached 67% of normal latency values for the infraorbital nerve and 70% for facial nerve latency values. Recently, a total osteocutaneous hemifacial allotransplantation model was developed in order to extend the application of the face/scalp transplantation in the rat model. This model included all hemifacial structures, such as vascularized nose, premaxilla, eyelids, and upper and lower lips, external ear, and facial skin. This new model, including all the hemifacial soft tissues as well as the premaxillary bone segment with nose components, enabled immunological, histological, and biological evaluation of different facial tissues and structures in one complex composite allotransplantation scenario. The most recent advancement in facial allotransplantation models is the development of composite face and eyeball allotransplant model with the optic nerve. This experimental model allows for evaluation of optic nerve regeneration and the effect of allotransplantation on composite facial tissues, including orbital content.