Craniofacial clefts include a complex and heterogenous group of deformities that affect the face, causing significant functional and appearance-related issues for affected patients. The term “rare” craniofacial cleft is used to differentiate them from the more “typical” clefts of the lip and palate. Fortunately, atypical facial clefts are exceptionally rare, with a reported incidence of 1.4–4.9 for every 100,000 births.
Etiology
Two theories predominate in establishing a cause of these deformities: the classic theory and mesodermal penetration theory. Whereas a failure of fusion of the developing facial processes is proposed by the former, the role of neural crest cells in the development of the mesoderm and its failed penetration is the central tenet of the mesodermal penetration theory.
There is increasing evidence that genetic predisposition plays a role in the pathogenesis of these rare craniofacial clefts. , The genetic component is more clearly evident in true midline clefts, further emphasizing the role of neural crest cells during embryogenesis. , Hu and Helms have demonstrated the critical role played by SHH (Sonic Hedgehog) signaling in regulating the pattern of neural crest cell migrations as well as the development of the facial primordium. The transient loss of SHH signaling during the initial phases of neural plate patterning has been linked to abnormalities of craniofacial morphogenesis, leading to anomalies resembling cleft lip/palate defects, hypotelorism, and holoprosencephaly. Excessive SHH signaling has been linked to mediolateral increment in the frontal process as well as hypertelorism.
Classification
The complexity and heterogeneity of facial clefts pose a challenge to classification. Two main classifications are currently utilized: Van der Meulen’s embryonic classification and the more widely used anatomical classification proposed by Tessier. , The latter delineates 14 locations for clefts, with the palpebral fissure as a central landmark, much like a wheel with spokes. Facial clefts extending downwards from the palpebral fissure are assigned the numbers 1 to 7, starting at the midline with Tessier 0 and each subsequent number representing a facial cleft more laterally positioned. Cranial clefts extending cephalad from the palpebral fissures are numbered 8 to 14, where Tessier 8 is the most lateral and extends into the corner of the orbit and each sequential cranial cleft is more medial than the last. Facial and cranial clefts may exist separate from one another or combined, at which point they become true “craniofacial clefts.” In such cases, the representative cleft numbers usually sum to 14 (e.g., 0,14; 3,11; 4,10) (see Fig. 19.1 ). , A number 30 cleft of the midline mandible is also included in the Tessier classification ( Fig. 19.1 ).
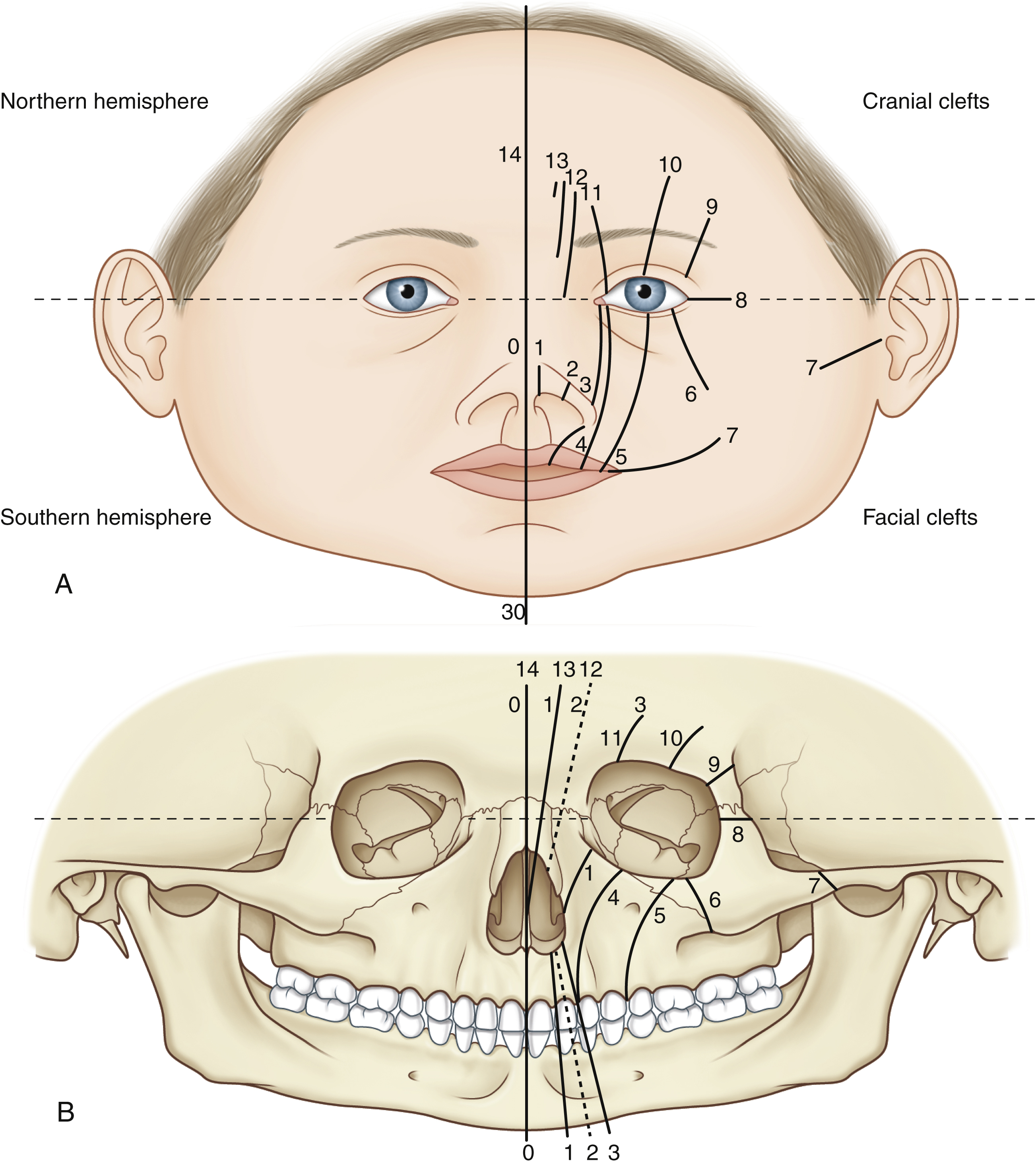
When clinically classifying facial clefts, a number of important anatomical distinctions should be identified to assist in the proper diagnosis. For example, nasal structures are involved only in clefts nos. 0–3, while no. 4 is the first to avoid the nose. Radiologically, no. 4 is visualized medial to the infraorbital foramen, while no. 5 is localized lateral to this structure ( Table 19.1 ).
The earliest documented history of facial clefts was first reported by Merkel and Trendelenburg, where they described facial clefts. However, Tessier illustrated a more detailed and systematic classification for craniofacial clefts that is widely accepted today. Tessier’s classification is unique given that it highlights the relationship between soft tissues and the underlying bone, stating that “a fissure of the soft tissue corresponds, as a general rule, with a cleft of the bony structure.” The converse is also possible. In addition, Tessier proposed the adoption of the term “cleft” for all craniofacial anomalies that fall along these lines, noting that there may be “excess” and/or “deficiency” clefts. Indeed, many surgeons consider both craniofacial microsomia and Treacher Collins syndrome as rare craniofacial clefts with variable amounts of soft tissue and bony involvement of the implicated Tessier cleft. For example, in craniofacial microsomia there may be a no. 7 cleft of the soft tissue associated with variable hypoplasia of the mandible whereas in Treacher Collins syndrome there may be a soft tissue cleft of nos. 6 or 7 and a hard tissue cleft of nos. 6, 7, and 8 or a combination thereof.
The main drawback of the Tessier classification is that it does not explain why clefts can occur at nonembryonic sites of fusion. While other authors have modified Tessier’s original classification, it continues to be the most widely utilized.
Van der Meulen’s embryological classification is considered by some to be more comprehensive as it attempts to explain why some clefts occur in areas unrelated to embryologic fusion. In this system the term “dysplasia” is used since not all malformations are true “clefts.” The dysplasias are classified according to time and location of developmental arrest (e.g., orbito-zygomatic dysplasia). Hypoplasia of the mandible is graded according to the Pruzansky classification and as adapted by Kaban et al. ,
Management
The management of facial clefts necessitates a multidisciplinary approach due to the involvement of multiple facial structures. Priorities remain airway and globe protection, followed by functional concerns such as the separation of nasal, orbital, and oral spaces, lip competence and eating. Furthermore, the treatment of craniofacial clefts necessitates the reconstruction of soft tissue and skeletal hypoplasia to obtain optimal esthetic improvement. It is important to note that there is no known, standardized “one-size fits all” surgical approach that can be constantly followed. This is because the majority of patients present with unique facial deformities within characteristic patterns of facial clefts. Even in extremely rare facial anomalies, the goal of the craniofacial surgeon is to get the desired result with fewest numbers of corrective surgeries.
Skin
Facial cleft deformities usually involve shortening of the facial dimensions along the cleft, leading to a “short oculo-oral distance.” The goal of soft tissue closure is to normalize the face’s vertical height, as well as to achieve repositioning of critical structures such as canthi, lower eyelids, lips and nose using traditional soft-tissue transposition techniques such as Z-plasties, back-cuts and/or rotation-advancements. Such repositioning must also incorporate excision of scarred tissues associated with the cleft.
Another important concept is the placement of scars to avoid the violation of anatomical facial units. In cases where the facial cleft involves a single-facial unit such as Tessier nos. 1, 2 or 5, a Z-plasty can be employed to provide esthetically acceptable lengthening and correction ( Fig. 19.2 ).
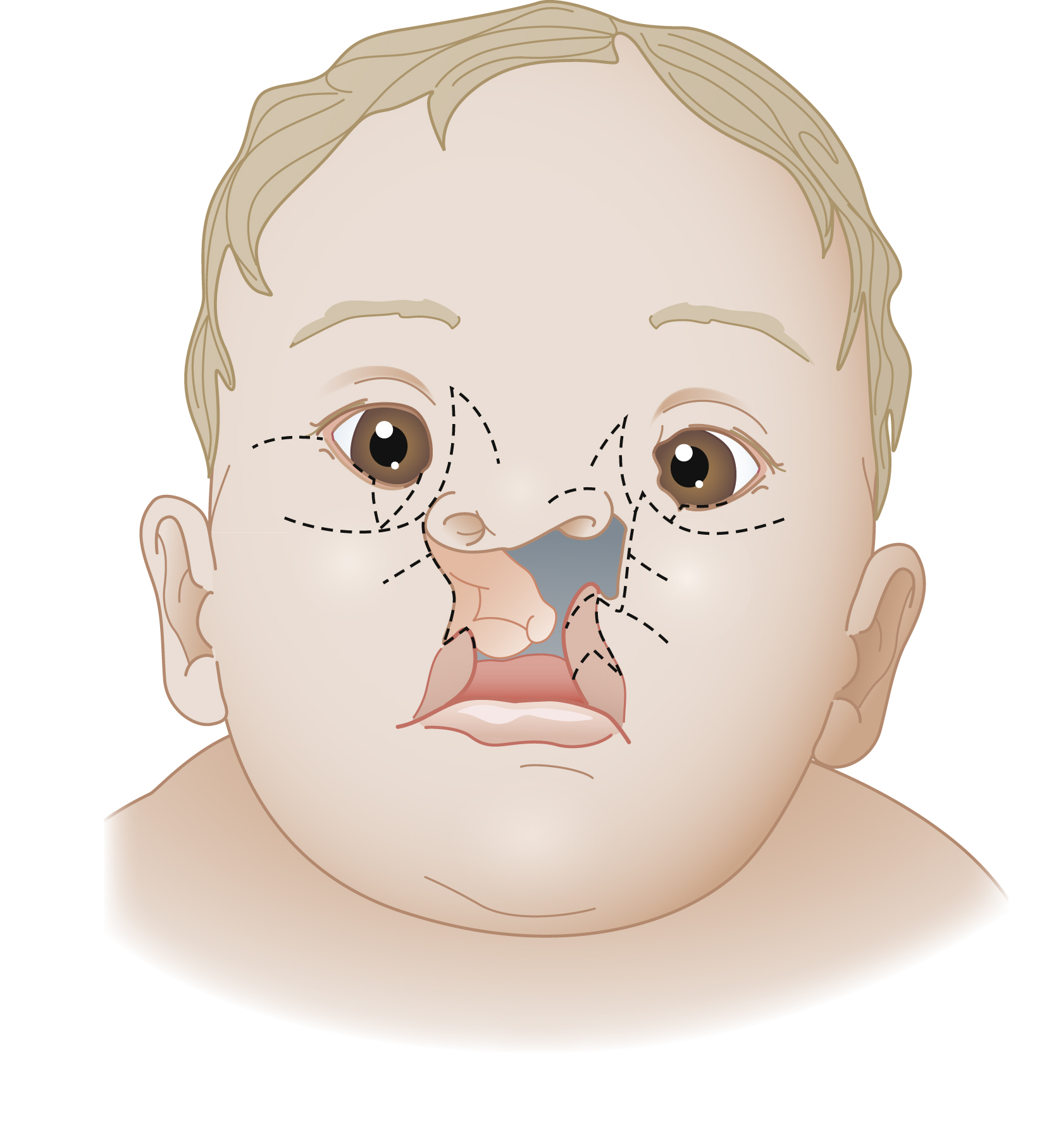
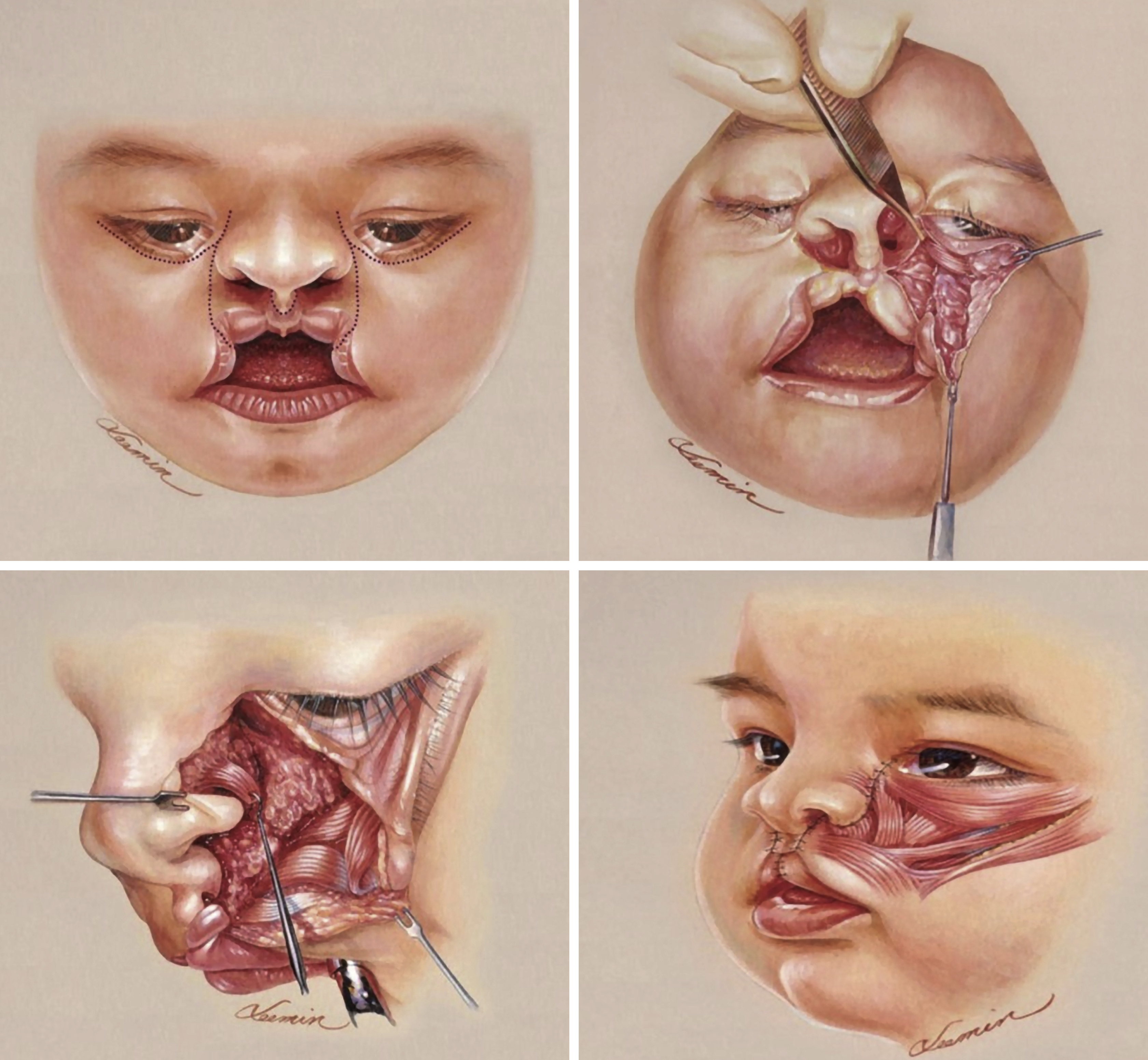
In facial clefts involving more than one facial unit, such as Tessiers 3 or 4, a midface rotation-advancement flap may provide superior esthetics to traditional interdigitating flaps or Z-plasties by limiting scars along the lines dividing subunits, as espoused by Chen et al. The authors also describe the importance of the realignment and repair of facial muscles, noting that it provided more natural facial expression and animation, as well as progressive lengthening of the initially vertically-deficient midface ( Box 19.1 and Fig. 19.3 ).
- •
Advancement of a laterally-based cheek flap
- •
A lateral canthotomy to gain more length and advance tissues medially toward the medial canthus, nose, and lip
- •
Rotation of a medially-based nasal flap
- •
Medial canthopexy
- •
Periosteal relaxing incisions lateral to infraorbital bundle to facilitate medial advancement of the cheek
- •
An orbicularis oculi flap is an integral component within the flap
- •
Repositioning and repair of the clefted facial expression muscles
- •
Placement of scars along the lines of the facial units
Attention must also be given to the mucosa at the time of skin repair as a significant portion of facial clefts are full-thickness. As in the more common clefts of the lip and palate, the mucosa is similarly closed using interdigitating flaps, Z-plasties, back-cuts, etc. Due to tissue deficiency which may be present, one may repair these defects initially with local flaps (rotation/advancement, back-cuts, Z-plasties), and then later in life transpose the scars to the boundary of the esthetic subunits with additional soft tissue flaps and/or tissue expansion to recruit additional tissue.
Eyelids
Colobomas are commonly associated with facial clefts involving the eyelids, characterized by a partial- or full-thickness defect. One of the key aims in determining the most appropriate type of reconstructive surgery is ensuring corneal protection. Artificial tears and ointments can be utilized, in addition to patching prior to surgical intervention for the eyelid reconstruction. Eyelid reconstruction can range from a simple repair or a minor modification procedure, to multiple complex surgical procedures involving flaps or grafts to achieve restoration of the anterior, middle, and posterior lamellae of the eyelid. It is often necessary to reposition the medial canthus either using a transnasal wiring technique or reattachment to the periosteum and is a crucial step in eyelid reconstruction. Sturdy reconstruction of the medial canthal complex is essential for appropriate lower eyelid support and to avoid inferior displacement. Lateral canthotomy can be used to assist medial translocation of the lid in cases where advancement is limited. Identification of the appropriate site is facilitated in unilateral cases by matching the unaffected side. Positioning is conversely more complex in bilateral cases, where estimation can be based on the relative position of the lateral canthus. Lastly, the planned medial canthal position should be 2 mm higher than the desired final location due to the tendency for inferior migration following skin repair. Appropriate assessment of the nasolacrimal system is required as it is often compromised in clefts involving the medial orbit. Dacryocystorhinostomy or a similar procedure at an interval may be required to restore appropriate lacrimal function.
Nose
Midline clefts can be accompanied by a nasal duplication, or alternatively an absence or excess of nasal structures. , Paramedian and/or oblique clefts frequently involve alar rim deformities, ranging from minor notching to malposition of the lateral crura, to total hypoplasia. Another variant, the proboscis, represents an embryonic remnant of a tubular nasal appendage. An encephalocele – also known as cranium bifidum – and hypertelorism can also be present. ,
Nasal reconstruction must encompass three-dimensional reconstruction of missing or deformed structures as well as preservation or reestablishment of nasal airway function. Evaluation of all nose components should be done in both a qualitative and quantitative manner in accordance with three aspects: skin, lining, and availability of cartilaginous or bony support. Prudent planning and careful assessment of all surgical options is necessary. Some defects require skeletal and soft tissue repairs before other anomalies can be addressed. This is especially true in nasal reconstruction, where correcting skeletal, soft tissue and orbital abnormalities often takes precedence to provide a stable platform for eventual nasal reconstruction. In other situations, such as midline or paramedian clefts involving orbital hypertelorism (e.g., frontonasal dysplasia) may undergo simultaneous correction of hypertelorism (four-wall osteotomy or facial bipartition) associated with cantilever bone grafting for reconstruction of the nasal dorsum and/or soft tissue excess excision.
Bony defects can be present along the cleft from the alveolus to the orbit. Autologous bone graft is the preferred material, in particular from rib, split calvarial or iliac crest donor sites. Midline and paramedial clefts may have nasal dorsum deformities or instability due to absent or deformed septal cartilage or splayed/absent nasal bones. Provided that a patient has septal nasal cartilage, it can be utilized as a graft for reconstruction of the caudal septum or nasal dorsum. Otherwise, costal cartilage can be harvested for more substantial and stable material. A composite chondromucosal flap based on the septal branch of the superior labial artery can also be utilized. The workhorse for bony nasal vault reconstruction remains a cantilever split cranial bone graft, combined often with osteotomies to medialize displaced nasal bones in cases of bifidity. Traditional cartilaginous tip suturing and support techniques, with or without grafts, for tip reshaping can be done simultaneously or at a later stage.
Minor deficiencies of the tip and alar rim can be addressed with the use of cartilage grafts or composite grafts (e.g., conchal) for deficient or notched alars ( Fig. 19.4 ). Alar repositioning is also essential and should be inferiorly overcorrected by 2 mm to account for the tendency for superior displacement.










