8 Vascular Anatomy of the Lower Extremity: A Practical Guide to Vascular Territories, Perforators, and Selection of Recipient Vessels
Summary
In order to choose the appropriate flap donor site or recipient vessels in lower extremity reconstruction, it is important to have an understanding of vascular architecture and anatomy of individual perforators in the region. The lower extremity has 21 vascular territories or angiosomes, and can be divided into four anatomic subregions: (1) gluteal, (2) hip and thigh, (3) knee and leg, and (4) ankle and foot. Within these regions, there are about 180 perforators to the integument, which are highly variable in caliber or location, although they tend to cluster about the main source arteries. Each perforator angiosome is linked to those adjacent by choke anastomotic or true anastomotic vessels, with a longitudinal or proximal-to-distal orientation. The dimensions of the available vascular territory supplied by an individual perforator depend on the size of that perforator, subregion, and unpredictable intrinsic patient factors. Since venous congestion is a well-known phenomenon occurring with perforator flaps, variations in venous anatomy should also be appreciated. Note that the lower limb is drained by both a superficial and a deep venous network, the latter usually the mirror image of the arteries that they accompany, which are interdependent and interconnected. Each source artery as well as its perforators can potentially serve as the recipient site for any microvascular tissue transfer.
Keywords: vascular anatomy, angiosome, perforator angiosome, choke vessel, microvascular recipient site
8.1 Introduction
This review of the vascular anatomy of the lower extremity is intended to emphasize the details of the anatomy of greatest interest to the reconstructive surgeon. Since the lower extremity is a common site for trauma and for reconstruction, knowledge of the vascular architecture of the lower limb is critical before deciding on an appropriate flap donor site or the planning of recipient vessels. The status of the main arterial supply to the lower extremity as well as the general pattern of individual perforators will be helpful in this regard.
8.2 Vascular Territories and the Angiosome Concept
Taylor and Palmer introduced the angiosome concept, which has been a guide to our understanding of the vascular territories of the human body.1 The word angiosome is derived from the Greek word angeion, which means vessel, and somite, which means segment of the body. The body can be divided into a series of angiosomes (vascular territories) based on the anatomy of the individual source artery to that angiosome. Each angiosome is a composite block of tissue all supplied by one main named source artery, and may consist of bone, muscle, fascia, and skin as well as other tissues. The main source vessel within the given angiosome gives off multiple branches or perforators, which in turn will be the vascular supply to each of its tissues. Individual angiosomes are linked to adjacent angiosomes via reduced caliber choke anastomotic vessels or true anastomotic vessels, which are subject to numerous physiologic influences (e.g., a delay procedure). The specific anatomy of a given angiosome and presence (or absence) of individual perforators or branches will then affect the survival of tissues harvested. A larger source artery with a larger angiosome and larger perforators may supply larger flaps and vice versa. The smallest division of the angiosome is that of an individual perforator that supplies a discrete region of tissue or perforator angiosome. The size of the vascular territory supplied by an individual perforator is dependent on a variety of factors including the size of the perforator, region of the body, and intrinsic patient factors, which may influence blood flow.
8.3 Arterial Territories
The integument of the human body can be divided into about 60 vascular territories that are supplied by about 400 perforators. However, the arterial framework of the body is actually a huge continuous interlocking arcade of vessels through all layers of all tissues. Arteries tend to give a branch to each structure they pass through, which has led to a myriad of terms such as fasciocutaneous, septocutaneous, and musculocutaneous perforators. The vessels that pierce the deep fascia and supply the skin may be direct, such as would be axial or septocutaneous perforators, or indirect, as those perforators which pass through other structures first en route to the skin such as would be musculocutaneous perforators. Note that there is roughly a 2/3:1/3 ratio of musculocutaneous to septocutaneous perforators throughout the body. The important point is to be able to identify the pattern of distribution of individual perforators in order to capture a suitable skin vascular territory in a flap.
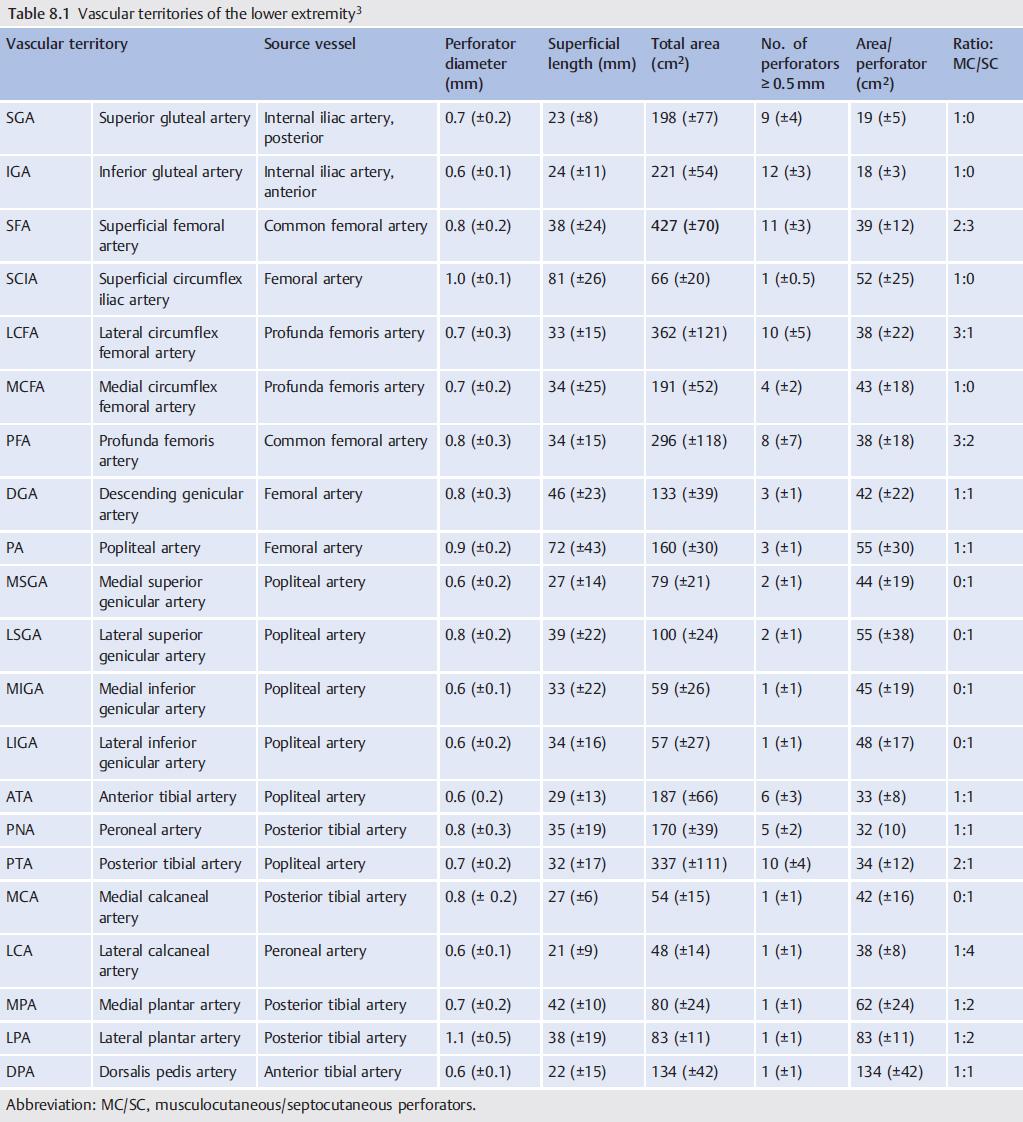
The lower extremity has 21 vascular territories with a mean of about 180 perforators (▶ Table 8.1).2,3 The location of these vascular territories in the lower extremity was summarized in a series of cadaver studies (▶ Fig. 8.1). As a rule, the named source vessels to these vascular territories are large consistent arteries with associated venae comitantes. These provide the vascular supply to numerous flaps in the body and also are available as recipient vessels for free microvascular tissue transfers. The individual cutaneous perforators to skin in the lower extremity are highly variable in terms of size and exact position, but tend to cluster around the main source vessels often with a longitudinal orientation, which allows some anticipation of their location.
8.4 Venous Drainage
The venous anatomy of the body has received relatively less attention, but is certainly equally important for successful reconstructive surgery. It is well known that perforator flap failure is often caused by venous insufficiency. The integument of the body is drained by a superficial and a deep venous network, which are interdependent and interconnected. The deep venous architecture generally mirrors that of the arterial tree and in most regions is duplicated. The superficial venous network is quite different and consists of long named venous channels that connect to the deep system via venae communicantes. Adjacent venous territories of the skin are interconnected via veins without valves, which are called oscillating or bidirectional veins (▶ Fig. 8.2).
8.5 Neurovascular Territories
The cutaneous nerves of the lower extremity are longitudinally arranged. Each cutaneous nerve is associated with an arterial supply that has a variety of orientations. For example, a series of small arterial branches can join the course of the nerve in a chain-linked pattern, or a single artery could run the full length of the nerve. In general, the cutaneous nerves have a well-vascularized longitudinal axis with indirect branches to the integument, which provides an opportunity to harvest local or regional neurocutaneous flaps (▶ Fig. 8.3).4
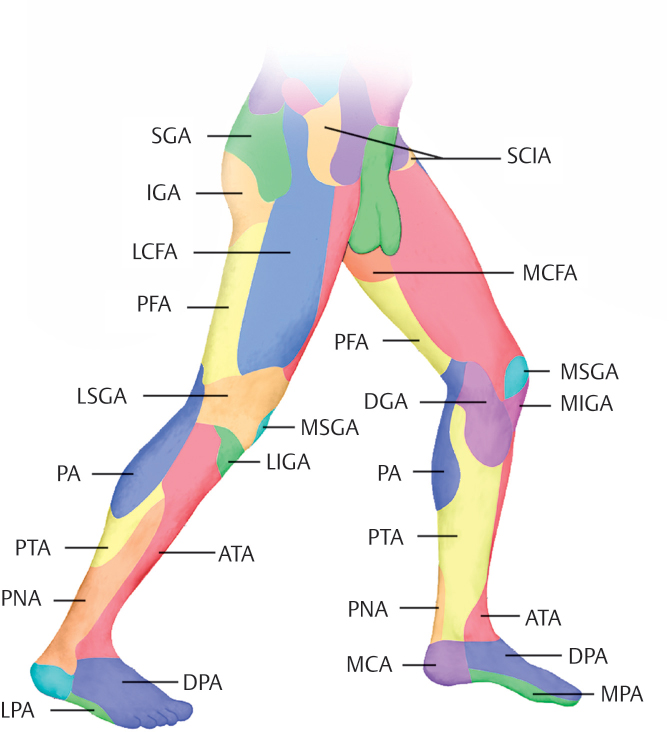
Fig. 8.1 Lower limb angiosomes derived from a series of angiograms in human cadavers. The vascular territories of the integument are shown in different colors according to the specific source artery. Abbreviations: ATA, anterior tibial artery; DGA, descending genicular [saphenous] artery; DPA, dorsalis pedis artery; FA, femoral artery; GT, greater trochanter; IGA, inferior gluteal artery; L, lateral epicondyle; LCA, lateral calcaneal artery; LCFA, lateral circumflex femoral artery; LIGA, lateral inferior genicular artery; LPA, lateral plantar artery; LSGA, lateral superior genicular artery; M, medial epicondyle; MCA, medial calcaneal artery; MCFA, medial circumflex femoral artery; MIGA, medial inferior genicular artery; MM, medial malleolus; MPA, medial plantar artery; MSGA, medial superior genicular artery; P, patella; PA, popliteal artery; PFA, profunda femoris artery; PNA, peroneal artery; PTA, posterior tibial artery; SCIA, superficial circumflex iliac artery; SGA, superior gluteal artery. (Adapted from Geddes CR, Tang M, Yang D, Morris SF. Anatomy of the lower extremity. In: Blondeel PN, Morris SF, Hallock GG, Neligan PC, eds. Perforator Flaps: Anatomy, Technique & Clinical Applications. St Louis, MO: Quality Medical Publishing; 2013:667–703.
8.6 Vascular Anatomical Principles Applied to Flap Design
For decades, surgeons relied on dogma such as the length-to-width ratio and trial and error to try to predict flap survival. The so-called random flaps were commonly utilized to reconstruct defects with unpredictable results. Fasciocutaneous and musculocutaneous flaps gradually replaced random flaps, as these had a more specific source of circulation that allowed more consistent and reliable results. The more recent enthusiasm for perforator flaps has focused the spotlight on detailed descriptions of the anatomy of individual cutaneous perforators throughout the body, and particularly the lower extremity so that flap survival has been improved.
In addition to knowing the anatomy of cutaneous perforators, an awareness of the physiologic effects on the vascular supply of tissues is important. Cormack and Lamberty described this as the anatomic, dynamic, and potential flap anatomy (▶ Fig. 8.4). A flap based on a single perforator will completely survive if designed to include only its perforator angiosome, or anatomic territory. A flap that includes that same perforator and an adjacent perforator should also completely survive via flow-through choke or true anastomoses, except when a compromising physiologic condition exists, which is the dynamic territory. Capture of a potential territory by inclusion of a second adjacent perforator territory is possible with a delay procedure or equivalent maneuver (▶ Fig. 8.5).
The variable nature of perforator distribution, size, and behavior throughout the body is particularly evident in the lower limb. In many regions of the lower extremity, perforator territories are small, and consequently, reliable flaps are smaller. In addition, physiologic challenges to the dynamic or potential surviving territory of a flap are commonplace, including vascular compromise due to diabetes or peripheral vascular disease, dependent edema, and trauma. Thus, it is not surprising that historically a 1:1 length-to-width ratio for a cutaneous flap in the lower extremity was the rule.
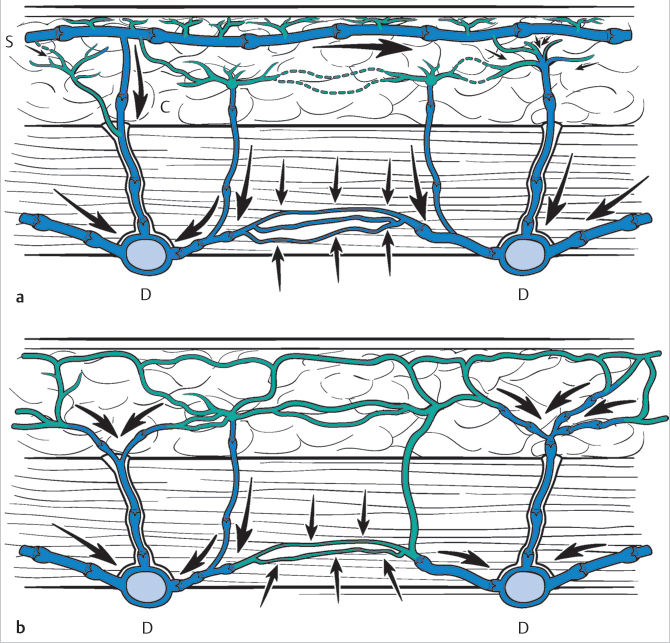
Fig. 8.2 Venous anatomy of the skin. (a) In the lower extremity, there are distinct superficial (S) and deep (D) venous networks that drain the skin and muscle. These are connected by valved venae communicantes (C), while venae comitantes provide secondary drainage. (b) Elsewhere in the body, there is only a deep system and venous drainage is predominantly from venae comitantes. In all areas of the body, oscillating veins (small arrows) link adjacent venous territories. (From Morris, SF, Davidson PG. Vascular basis of flaps and flap classification. In: Zenn MR, Jones G, eds. Reconstructive Surgery. Anatomy, Technique, and Clinical Applications. New York, NY: Thieme; 2012:35–80.)
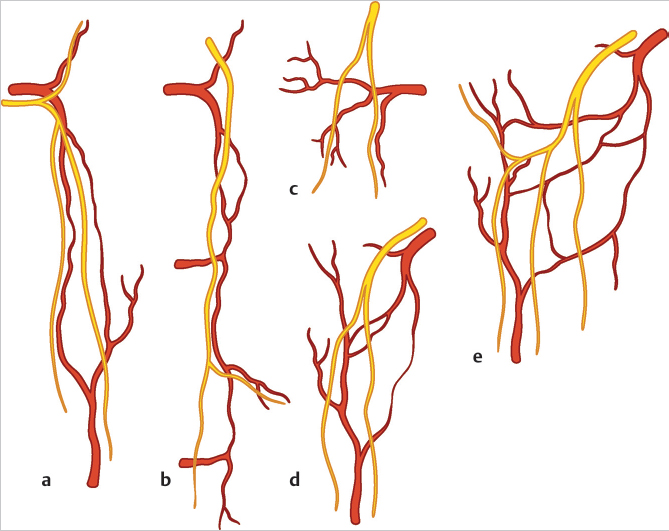
Fig. 8.3 The neurovascular patterns of the integument. (a) A long artery courses with the nerve, and here in addition there is a true anastomosis between perforator angiosomes. (b) A system of multiple arteries “hitchhike” with the nerve. (c) A nerve and artery pierce the fascia at separate sites, but unite distally. (d) A nerve diverges from its accompany artery and then descends toward the main trunk of another artery. (e) A nerve crosses the primary and secondary vascular arcades to then travel parallel to another artery. (From Morris, SF, Davidson PG. Vascular basis of flaps and flap classification. In: Zenn MR, Jones G, eds. Reconstructive Surgery. Anatomy, Technique, and Clinical Applications. New York, NY: Thieme; 2012:35–80.)
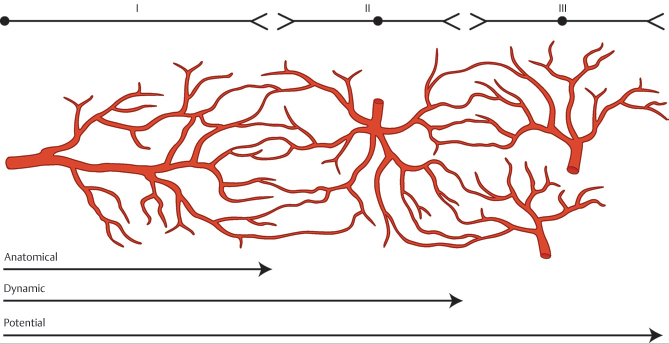
Fig. 8.4 Cormack and Lamberty’s concept of the anatomic, dynamic and potential territories of flap design. (From Morris, SF, Davidson PG. Vascular basis of flaps and flap classification. In: Zenn MR, Jones G, eds. Reconstructive Surgery. Anatomy, Technique, and Clinical Applications. New York, NY: Thieme; 2012:35–80.)
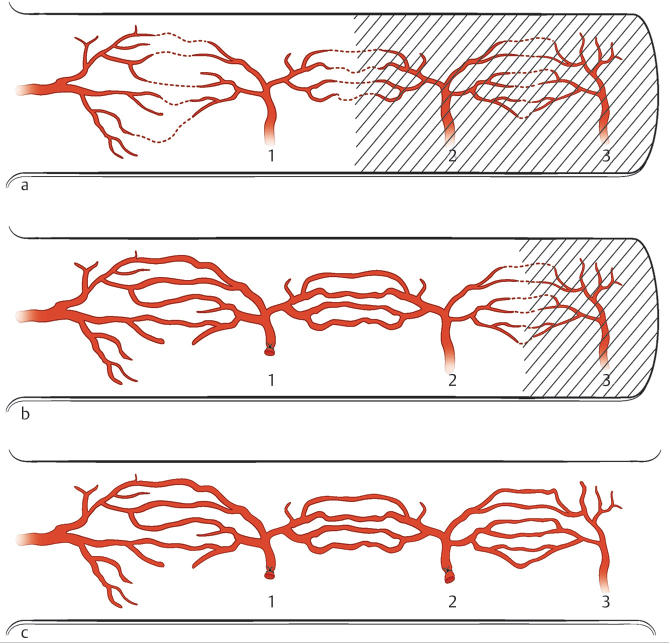
Fig. 8.5 (a) Flap elevated on a single perforator and including only the next perforator territory will completely survive consistently. (b) After delay of the next adjacent perforator angiosome, a flap will reliably and consistently survive including two territories. (c) A delay of perforators 1 and 2 will result in a large three-territory flap completely surviving. The shaded area represents flap necrosis. (From Morris, SF, Davidson PG. Vascular basis of flaps and flap classification. In: Zenn MR, Jones G, eds. Reconstructive Surgery. Anatomy, Technique, and Clinical Applications. New York, NY: Thieme; 2012:35–80.)
8.7 Main Source Vessels of the Lower Extremity
8.7.1 Arterial System
The blood supply to the lower extremity is predominantly a continuation of the external iliac, which proceeds all the way to the foot with name changes as it passes defined landmarks. After the external iliac enters the thigh deep to the inguinal ligament, it is referred to as the common femoral artery (FA). This continues as the superficial FA, popliteal artery (PA), tibioperoneal trunk, posterior tibial artery (PTA), and, ultimately, terminates as the medial and lateral plantar arteries (▶ Table 8.2). The other well-known arteries of the lower limb are branches arising from this main trunk (▶ Fig. 8.6).
The internal iliac artery also has a small contribution to the lower extremity via the gluteal vessels (superior and inferior), which are its terminal branches. The gluteal arteries supply the buttocks and form an anastomoses in the posterior thigh with the medial and lateral circumflex femoral vessels.
8.7.2 Venous System
The lower extremity circulation is drained by two venous systems: the superficial and the deep veins. The deep venous system travels with and is named after the arteries that it accompanies, as described previously. The superficial venous system has two dominant veins: the great saphenous vein and the small saphenous veins, both of which run in the subcutaneous tissue (▶ Fig. 8.6). The greater saphenous vein is found medially, arising from the foot, passing anterior to the medial malleolus, and then traveling superiorly, to eventually enter the femoral triangle through the fossa ovalis to join the femoral vein. Through most of its course distal to the adductor canal of the thigh, it is accompanied by the saphenous nerve. The lateral portion of the foot and leg is supplied by the small saphenous vein, which exits the foot posterior to the lateral malleolus and then travels superiorly to pierce the crural fascia at a variable location to follow between the two heads of the gastrocnemius muscle until usually emptying into the popliteal vein. The sural nerve usually becomes superficial at the mid-calf level to join the small saphenous vein.
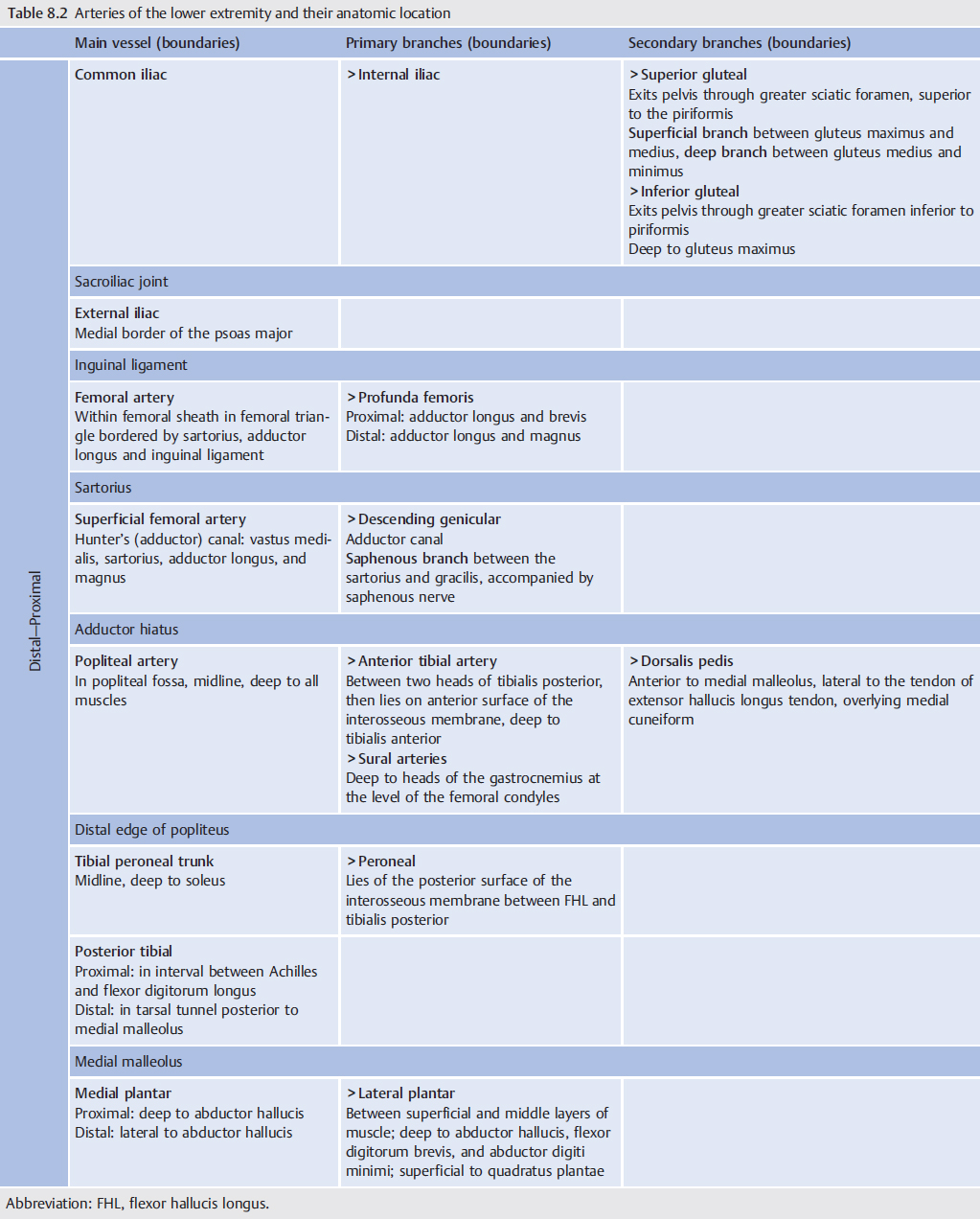
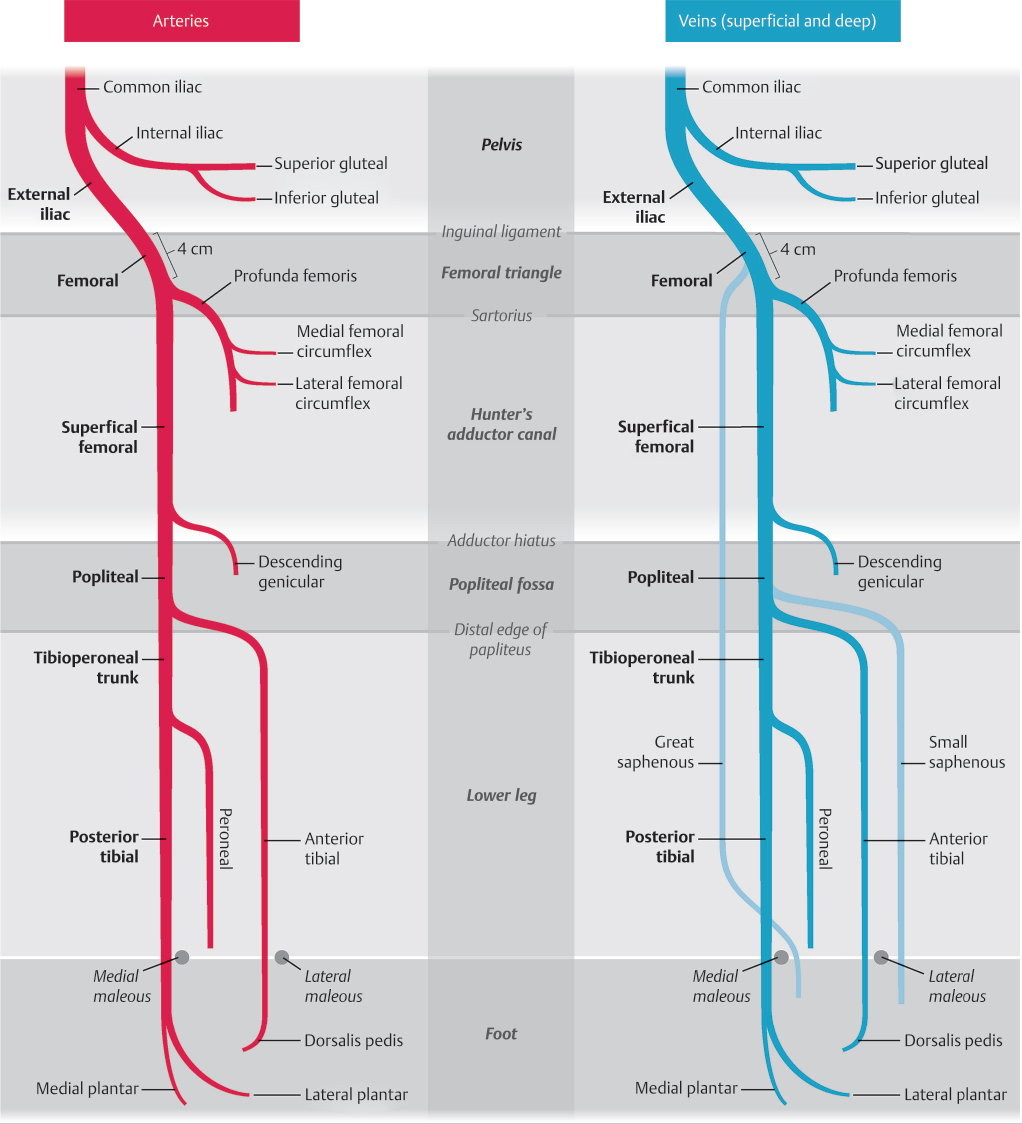
Fig. 8.6 Schematic diagram of the arterial and venous anatomy of the lower extremity showing important related anatomic landmarks.
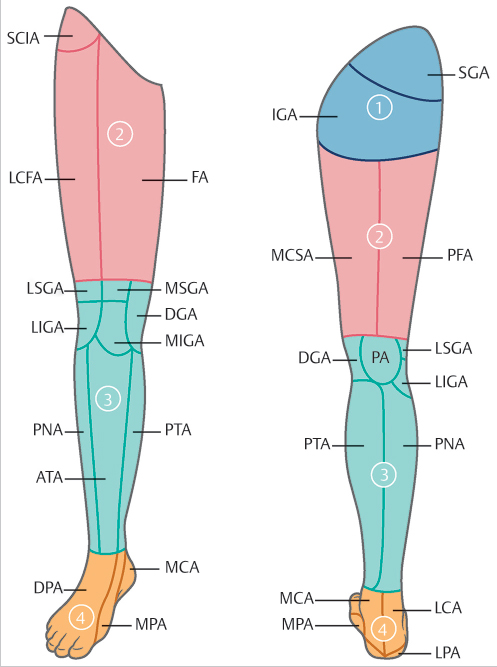
Fig. 8.7 The lower extremity can be divided into four anatomic subregions: (1) gluteal, (2) hip and thigh, (3) knee and leg, and (4) ankle and foot. Within these regions, there are 21 cutaneous vascular territories. See ▶ Table 8.1 to explain acronyms.
8.8 Regional Anatomy of Perforators of the Lower Extremity
Topographically, the lower extremity can be divided into four anatomic subregions: (1) gluteal, (2) hip and thigh, (3) knee and leg, and (4) ankle and foot (▶ Fig. 8.7). Within these subregions, there are 21 cutaneous vascular territories (▶ Fig. 8.1). The main source vessels are listed, and perforators in each major vascular territory can be described in terms of the area, size, location, and perforator course from the skin to the source vessel (▶ Table 8.1). Each source artery or its perforators could be potentially used to supply or serve as recipient vessels in microsurgical reconstruction of the lower extremity. In the following sections, perforators are described from their cutaneous location back to their source vessel.
8.9 Anatomical Regions
8.9.1 Gluteal Region
Introduction
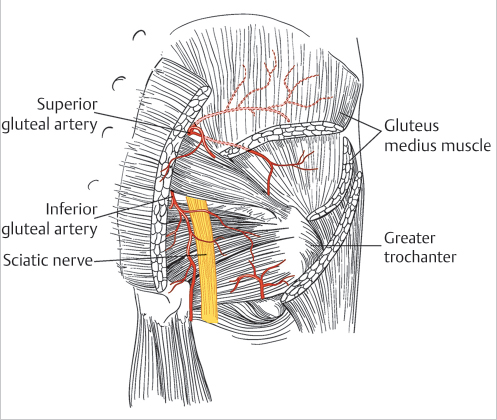
The gluteal region extends from the iliac crest to the gluteal fold, posterior midline, and a line intersecting the anterior superior iliac spine and the greater trochanter. In total, the gluteal region constitutes 12% of the surface area of the lower extremity. The two main source arteries are the superior and inferior gluteal arteries (▶ Fig. 8.8). There are minor contributions from the fourth lumbar artery, lateral sacral artery, the internal pudendal artery, and the ascending branch of the lateral femoral circumflex artery (LCFA).
Related posts:
 General Wound Preparation and Timing
General Wound Preparation and Timing
 The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
 Supermicrosurgery Approach to the Lower Limb
Supermicrosurgery Approach to the Lower Limb
 Nonflap Wound Closure Alternatives: Skin Graft, Skin Substitute, Skin Stretch, and Negative-Pressure Wound Therapy
Nonflap Wound Closure Alternatives: Skin Graft, Skin Substitute, Skin Stretch, and Negative-Pressure Wound Therapy
 Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
 Procurement of Thin Flaps as Indicated in the Lower Extremity
Procurement of Thin Flaps as Indicated in the Lower Extremity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


