12 Nonflap Wound Closure Alternatives: Skin Graft, Skin Substitute, Skin Stretch, and Negative-Pressure Wound Therapy
Summary
The evolution of wound closure techniques has introduced different alternative methods of closing the wound. Nonflap-wound-closure methods can be applied to cover many types of the wound. Negative-pressure wound therapy has changed the way we approach reconstruction in terms of preparation and closure for some defects. Skin substitutes allow faster granulation and skin stretch devices allow us to close small wounds that are ambiguous for reconstruction. This chapter covers these alternative methods of healing wound. This chapter covers these alternative supporting approaches.
Keywords: negative-pressure wound therapy, skin stretching device, skin substitutes
12.1 Introduction
The skin is the largest organ of the human body with a surface area of 1.2 to 2.0 m2 and 8% of total body weight.1 The skin protects the body from pathogens and excessive water loss. It also controls body temperature, senses external stimuli, blocks ultraviolet rays, and serves an aesthetic function. It is a complex organ consisting of epidermis and dermis including hair follicle, sensory nerve, and sweat gland. When injury to the skin is deep to the dermis and the apocrine glands and the pilosebaceous unit is destroyed, the skin loses its generative capacity.2
The use of modalities of secondary healing with negative-pressure wound therapy (NPWT), primary closure, and skin graft is located at the lower part of the traditional reconstructive ladder.3 Although it is at the lower step of the ladder, it can cause more complications than the modalities that is at the upper rungs of the ladder when the method is applied to the improper condition of the wound.
A small wound can be healed by secondary intention by wound contraction and epithelization from the wound margin. However, if the defect is full thickness and wide, it takes a long time to heal and eventually makes a wide scar with deformity and sometimes it becomes a nonhealing wound. Even when we close the wound with a primary suture, it does not heal well due to its tension and also produces unsightly scars. Therefore, if the wound is wide, skin graft or flap must be used to cover the wound.
Skin graft is the most common and simplest way to cover a superficial defect. The origin of the skin graft is an ancient technique. It was performed as early as 2500 BC to cover nasal skin defect.4 Then, over the next few thousand years, only a few anecdotal descriptions report the use of grafts to cover the traumatic defects. In Bologna, in his famous treatise on medicine of 1597, Gaspare Tagliacozzi (1545–1599) mentions a cutaneous transplantation.5 Although skin grafting has been known for centuries, it was not until the 19th century that grafting was rediscovered, improved, and then generalized.6,7,8
Skin grafts are indicated for covering of skin defect caused by trauma, burn, after excision of tumor, in case the primary closure of the defect is not possible, and wound bed is well granulated and vascularized.
12.2 Negative-Pressure Wound Therapy
NPWT is used for almost all wounds including pressure sores, soft-tissue injuries caused by trauma, burns, diabetic foot, and postoperative wounds. Despite its universal use of NPWT, there are still no randomized clinical trials (RCT) with high-certainty evidence that demonstrates its superior efficacy over conventional dressing,9,10,11,12,13 but only few people suspect its efficacy. NPWT is being used for an increasingly wide range of applications with the primary purpose of promoting granulation tissue formation.
12.2.1 Indications of NPWT in Open Wounds
NPWT can be used for the following indications:
• Deep open wound.
• Wound bed preparation (▶ Fig. 12.1, ▶ Fig. 12.2):
◦ Before split-thickness skin graft (STSG) or flap surgery.
• During the infected wound management:
◦ Instillation system can be used.
◦ Surgical wound dehiscence.
• If neither primary closure nor flap surgery is possible.
12.2.2 Protocols of NPWT for the Infected Wound with Necrotic Tissue
NPWT is a very effective method to remove a large amount of discharge and minimize the bacterial burden of the wound. During the early period of wound management for the infected wound with massive necrotic tissue, serial surgical debridement is needed along with proper antibiotics use and dressing. In between the serial debridement, NPWT can be applied as a wound dressing method. For infected wound, NPWT with instillation is better than standard NPWT,14,15 and as an instillation solution, normal saline solution is as effective as other antiseptics.16,17

Fig. 12.1 (a) Necrotic tissue and biofilm remaining after first debridement of dog bite wound. (b) After applying negative-pressure wound therapy for the wound for a week, and (c) wound coverage with free perforator flap.
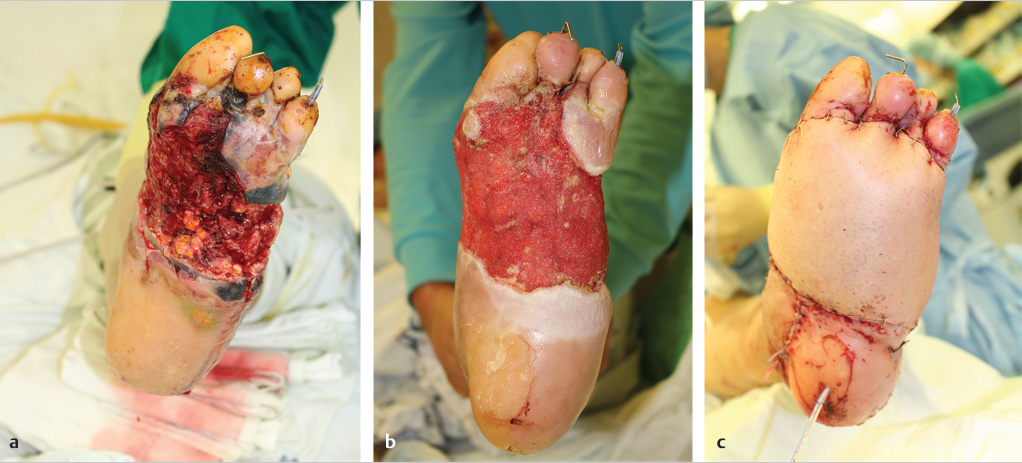
Fig. 12.2 (a) Necrotic tissue was seen on the surface after initial debridement. (b) Healthy granulation tissue was covering the surface following serial debridement and negative-pressure wound therapy after 11 days after initial debridement. (c) The wound was covered with free perforator flap.
12.2.3 Limitations
NPWT is only a dressing method bridging in between the surgical debridement. NPWT cannot replace scheduled wound evaluation or any surgical procedure including necrotic tissue removal and pus drainage. For example, in the early phase of infected diabetic wound care, daily surgical debridement is needed in the severely infected limb. The duration in between the debridement can be modified based on the condition of the wound.
12.2.4 Pitfalls of Negative-Pressure Wound Therapy
NPWT undoubtedly has the advantage of growing granulation tissue. Sometimes wounds that previously only could be covered with flaps can also be covered with secondary healing or skin grafts after using NPWT. As some of the reports could be easily found,18,19,20,21,22 more and more people are using NPWT for deeper wounds. In some wounds with exposed bone or ligament, NPWT may make it covered by the granulation tissue and, finally, STSG could be applied with cosmetically or functionally undesirable result. If there was no sufficient granulation even after weeks of NPWT, eventually flap coverage is needed, which is already delayed and the cost of the wound care is inevitably increasing.
12.3 Split-Thickness Skin Graft
The recipient bed should have good vascular supply, with no devitalized tissue. Skin graft take is possible over the healthy granulation tissue, fat, muscle, and fascia, but skin graft will be necrotized over the cartilage or bone without periosteum or perichondrium and tendon without paratenon due to lack of nutrition. However, even if there is no vascular distribution, skin grafts can survive if the defective skin area is narrow. Up to a distance of 0.5 cm from the edge of the skin defect, the skin graft can be nourished by the bridge.23 In practice, 0.5-cm-width cartilage or tendon without paratenon and perichondrium can be covered by skin graft alone. If there is a necrotic tissue in the recipient site, surgical debridement is needed. After the removal of the necrotic tissue, thorough hemostasis is essential. After debridement, a skin graft can be delayed until the granulation covers the defect.
12.3.1 Flap versus Skin Graft
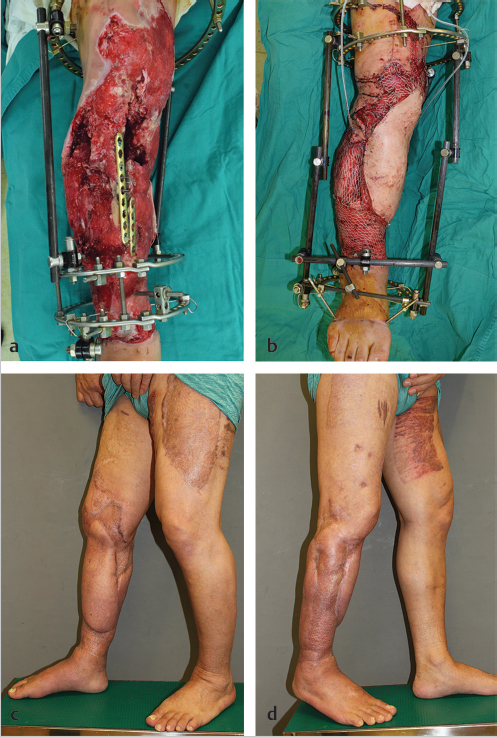
The choice between skin graft and flap depends mainly on recipient status, defect size, location, and postsurgery aesthetics. The success of skin graft depends on the vascular status of the recipient site. A well-vascularized bed is the best indication for skin graft. In the cases where the bone or the implants are exposed or dead space in the defect is large, free tissue transfer or local flap, including propeller flap, is essential to fill and cover the defect (▶ Fig. 12.3).
Related posts:
 General Wound Preparation and Timing
General Wound Preparation and Timing
 The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
 Supermicrosurgery Approach to the Lower Limb
Supermicrosurgery Approach to the Lower Limb
 Lower Limb Vascularized Composite Allotransplantation
Lower Limb Vascularized Composite Allotransplantation
 Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
 Procurement of Thin Flaps as Indicated in the Lower Extremity
Procurement of Thin Flaps as Indicated in the Lower Extremity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


