Abstract
Urticaria is characterized by transient skin or mucosal swellings due to plasma leakage. When the swelling is superficial within the dermis, pruritic wheals appear, whereas when deep, angioedema is seen. While urticaria often develop in the setting of anaphylaxis, patients who present with wheals rarely progress to anaphylaxis. Urticaria may be spontaneous or inducible, as well as acute or chronic. Acute spontaneous urticaria can have an allergic basis, but chronic spontaneous urticaria (CSU) usually does not. Although there is circumstantial evidence for an autoimmune etiology in approximately one-third of patients with CSU, many cases remain unexplained, i.e. are idiopathic. Nonsteroidal anti-inflammatory drugs, foods, alcohol, stress, and infections may aggravate CSU, but they are rarely the cause. Although inducible urticarias are defined based upon their trigger(s), the cause is unknown, with the exception of contact urticaria. The primary effector cell of urticaria is the mast cell, and histamine from mast cells is the major mediator of pruritus and wheals. Angioedema is usually due to release of mast cell mediators, but may be mediated by bradykinin if the angioedema is not accompanied by wheals as in hereditary angioedema and angiotensin-converting enzyme (ACE) inhibitor-induced angioedema. H1 antihistamines are the primary treatment of urticaria. Oral corticosteroids should only be used when rescue therapy is required. Immunosuppressives or omalizumab (anti-IgE antibody) are third-line options for H1 antihistamine-refractory CSU.
Keywords
urticaria, spontaneous urticaria, inducible urticaria, acute urticaria, chronic urticaria, autoimmune urticaria, chronic spontaneous urticaria, angioedema, hereditary angioedema, angiotensin converting enzyme (ACE) inhibitor-induced angioedema, histamine, bradykinin, H1 antihistamine, omalizumab
- ▪
Urticaria is characterized by transient skin or mucosal swellings due to plasma leakage. Superficial dermal swellings are wheals, and deep swellings of the skin or mucosa are termed angioedema. Wheals are characteristically pruritic and pink or pale in the center, whereas angioedema is often painful, less well-defined, and shows no color change
- ▪
There are several recognizable clinical patterns of urticaria and different causes. The latter include allergy, autoimmunity, drugs, dietary pseudoallergens, and infections. Many cases of spontaneous urticaria remain unexplained (“idiopathic”) even after an extensive evaluation. C1 esterase inhibitor deficiency needs to be considered as a cause of recurrent angioedema without wheals
- ▪
Diagnosis is based primarily on the history and clinical examination. Determination of the etiology or triggers, as well as exclusion of other diagnoses, may require further investigations, including blood tests, physical and dietary challenges, skin tests, and skin biopsy
- ▪
Urticaria is a common disorder that may cause considerable distress and last for years, but the symptoms can usually be alleviated by appropriate management
Introduction
Urticaria is a common reason for patients to present to primary care practitioners, emergency rooms, dermatologists, and allergists. It is characterized by the rapidity of its fluctuation. As a rule, individual wheals last no more than 24 hours, but the entire affliction usually lasts much longer. With nearly all clinical patterns of urticaria, wheals may be accompanied by angioedema, but the occurrence of isolated angioedema (without wheals) is of special significance because some of these patients will have a deficiency of C1 esterase inhibitor (C1 inh). The latter is due to bradykinin formation rather than release of mast cell mediators. C1 inh deficiency is a rare disorder that is often inherited and because it can prove fatal without treatment must be considered in any patient with isolated angioedema. Urticarial vasculitis is an important disorder to exclude in patients with chronic urticaria. It is a systemic disease defined by damage to small blood vessels rather than transient vasodilation and vascular permeability (see Ch. 24 ). Urticarial vasculitis sometimes presents with wheals or angioedema that, without confirming a duration of more than 24 hours (by serial examination of marked lesions) and a lesional skin biopsy, are indistinguishable from other patterns of urticaria. While urticaria rarely progresses to anaphylaxis, wheals are often a feature of that condition. Good management of urticaria depends on a thorough understanding of etiologies, triggers and aggravating factors, in addition to the most appropriate drug therapies.
Definition of Urticaria
Urticaria is often used as a descriptive term for recurrent whealing of the skin, with angioedema being viewed as a physical sign. However, there is increasing acceptance that the term “urticaria” is more appropriately used to define a disease that may be acute or chronic. Thus, urticaria may present with wheals, angioedema, or both.
Wheals are pruritic, pink or pale swellings of the superficial dermis that have an initial erythematous flare around them ( Fig. 18.1 ). Lesions may be a few millimeters in diameter or as large as a hand, and the number can vary from a few to numerous. The hallmark of wheals is that individual lesions come and go rapidly, by definition, generally within 24 hours.

Angioedema swellings occur deeper in the dermis and in the subcutaneous or submucosal tissue. They may also affect the oropharynx and rarely the bowel in hereditary angioedema. The areas of involvement tend to be normal or faint pink in color, painful rather than pruritic, larger and less well-defined than wheals, and they often last for 2 to 3 days ( Fig. 18.2 ).

Epidemiology
Depending on the age range and method of sampling, estimates of the lifetime prevalence of urticaria in the general population range from 8 to 22% , with chronic urticaria ranging from 2 to 3% and having a point prevalence of 0.1–0.9%; the prevalence of specific subtypes of chronic urticaria, e.g. the inducible urticarias, is lower. Urticaria is a worldwide disease and may present at any age. The peak incidence depends on etiology. The proportion of cases due to different etiologic agents is likely to relate to the frequency of environmental exposures, such as infections and allergens, in different countries, but estimates of this are not available. It is also often difficult to prove a cause and effect, and so an underlying condition may be inappropriately “blamed” for causing urticaria. Overall, urticaria is more common in women, with a female : male ratio of ~2 : 1 for chronic spontaneous urticaria, but the ratio varies with the different physical urticarias. For example, women outnumber men in dermographism and cold urticaria, but more men develop delayed pressure urticaria . Hereditary angioedema has an autosomal dominant inheritance pattern and occurs in ~1 in 50 000 individuals, with a range that varies from 1 in 20 000 to 1 in 60 000.
Pathogenesis
The Mast Cell
Distribution and diversity
The mast cell is the primary effector cell of urticaria. Mast cells are widely distributed throughout the body but vary in their phenotype and response to stimulation. This may explain why systemic features, such as those seen in anaphylaxis, do not accompany the activation of cutaneous mast cells in urticaria. The majority of mast cells in the skin and intestinal submucosa contain the neutral proteases tryptase and chymase (MC TC ), whereas those in the bowel mucosa, alveolar wall, and nasal mucosa contain only tryptase (MC T ). Both types, however, express high-affinity IgE receptors (FcεRI) and are therefore capable of participating in IgE-dependent allergic reactions . There is conflicting evidence on the number of cutaneous mast cells in chronic urticaria, but there is agreement that they may be more likely to degranulate in response to certain stimuli, such as intradermal codeine injection , and in this sense may be in general more “releasable” . Little is known about the beneficial effects of mast cells, but there is some evidence that they may be involved in the innate immune response to infection, wound healing, and the neuroendocrine system. They have also been shown to help initiate the extracellular matrix formation and angiogenesis required for neurofibroma development (see Fig. 61.2 ).
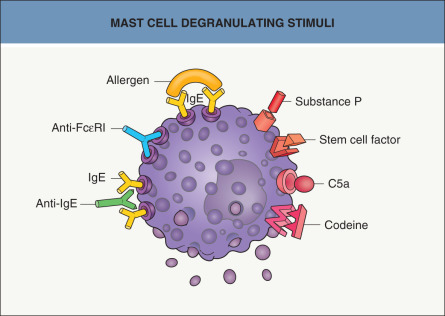
Degranulating stimuli
Cross-linking of two or more adjacent FcεRI on the mast cell membrane will initiate a chain of calcium- and energy-dependent steps leading to fusion of storage granules with the cell membrane and externalization of their contents. This is known as degranulation. Classic immediate hypersensitivity reactions involve binding of receptor-bound specific IgE by allergen. There are also several recognized immunologic degranulating stimuli that act through the IgE receptor, such as anti-IgE and anti-FcεRI antibodies ( Fig. 18.3 ). However, not all autoantibodies with these specificities are functional, i.e. capable of releasing histamine from mast cells or basophils in vitro . In addition, because functional anti-IgE and anti-FcεRI autoantibodies have been identified in patients with other diseases such as systemic lupus erythematosus and occasionally in healthy controls, the role of functional autoantibodies in the pathogenesis of urticaria has been debated. Non-immunologic stimuli, including opiates, C5a anaphylatoxin, stem cell factor, and some neuropeptides (e.g. substance P), can cause mast cell degranulation by binding specific receptors, independent of the FcεRI (see Fig. 18.3 ).
Proinflammatory mediators
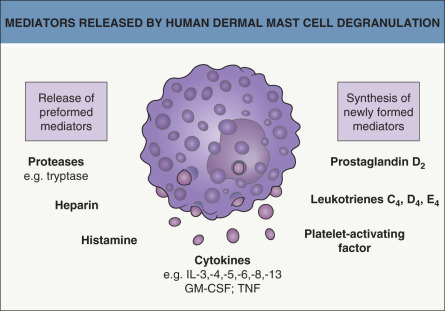
Mast cell granules contain preformed mediators of inflammation, the most important of which is histamine ( Fig. 18.4 ). A wide range of cytokines has been identified in human mast cells from different tissues, including tumor necrosis factor (TNF), interleukins (IL)-3, -5, -6, -8 and -13, and granulocyte–macrophage colony-stimulating factor (GM-CSF). Synthesis and secretion are upregulated following FcεRI stimulation. TNF is expressed constitutively in resting human cutaneous mast cells. Prostaglandins and leukotrienes are synthesized from arachidonic acid derived from cell membrane phospholipids (see Fig. 130.6 ). The most important proinflammatory eicosanoids are prostaglandin (PG) D 2 and the leukotrienes (LT) C 4 , D 4 , and E 4 (slow releasing substance of anaphylaxis). PGE 2 has inhibitory effects on immunologic mast cell degranulation and may therefore have a protective role in urticaria. Increased levels of TNF, IL-1β, -6, -10, -12p70, -13, and B-cell activating factor (BAFF) have been detected in the sera of urticaria patients .
Blood Vessels
Histamine and other proinflammatory mediators released upon degranulation bind receptors on postcapillary venules in the skin, leading to vasodilation and increased permeability to large plasma proteins, including albumin and immunoglobulins. Furthermore, histamine, TNF, and IL-8 upregulate the expression of adhesion molecules on endothelial cells, thereby promoting the migration of circulating inflammatory cells including eosinophils, basophils, neutrophils and Th0 cells from the blood into the urticarial lesion .
Blood
Autoantibodies
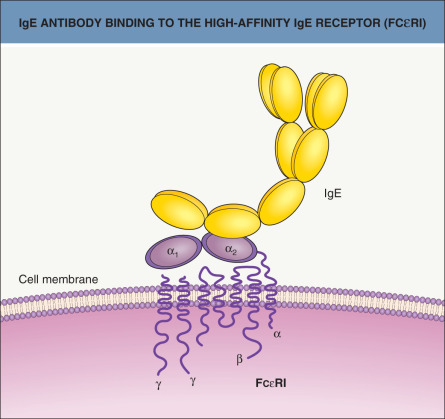
Based upon in vitro assays, functional IgG autoantibodies that release histamine (and other mediators) from mast cells and basophils have been detected in the serum of 30–50% of patients with chronic spontaneous urticaria (CSU) . The majority of these autoantibodies bind the extracellular α subunit of FcεRI. Those recognizing the α 2 domain compete with IgE for the binding site, whereas non-competitive autoantibodies directed against the terminal α 1 domain are able to bind the receptor in the presence of IgE ( Fig. 18.5 ). Approximately 10% of chronic urticaria sera contain functional autoantibodies directed against the Fc portion of IgE itself (see Fig. 18.3 ). Binding of the autoantibodies to mast cells may initiate complement activation with the generation of C5a anaphylatoxin, which in turn facilitates or augments degranulation . Other mast cell activating factors may also exist in urticaria sera, e.g. a non-IgG “mast cell-specific factor” has been described, although its identity remains unknown . There is currently no evidence that characterized cytokines cause mast cell degranulation in urticaria. Evidence from small series of CSU patients treated with plasmapheresis or cyclosporine indicates that functional autoantibody levels correspond to disease severity.
Leukocytes
The importance of peripheral blood leukocytes in the pathogenesis of urticaria is becoming clearer. Blood basophils in CSU patients are less responsive in vitro to the immunologic stimulus anti-IgE, possibly through desensitization, and these cells are reduced in number . These patients can be further classified into responders and non-responders based upon the release of histamine by their basophils in response to anti-IgE. The functional phenotype appears to remain stable during the course of the active illness, but then, during disease remission, the basophils become more responsive to anti-IgE . Expression of the negative regulator SHIP (src homology 2-containing inositol phosphatase) is increased in the basophils from anti-IgE non-responders , although the significance of this to the pathogenesis of chronic urticaria is unknown. Evidence has emerged that basophils are recruited into urticarial wheals and may sustain the inflammatory response by releasing histamine and other mediators, analogous to the delayed phase of immediate hypersensitivity reactions.
Eosinophil, neutrophil, and lymphocyte numbers are normal in the peripheral blood, but these cells are often present in biopsy specimens from spontaneous wheals. Eosinophils may contribute to the persistence of wheals by generating LTC 4 , LTD 4 , and LTE 4 and by releasing toxic granule proteins, including major basic protein (MBP), which can release histamine from basophils. The function of neutrophils and lymphocytes in urticaria has not been elucidated.
Nerves
Substance P and other neuropeptides release histamine from mast cells in vitro and can induce a wheal and flare reaction in human skin when injected intradermally. Vasoactive intestinal polypeptide (VIP) caused a greater wheal reaction in those with chronic urticaria than did other skin-tested neuropeptides, but the relevance of this to urticaria is still uncertain.
Mechanisms of Urticaria Formation
Mast cell-dependent urticaria
Potential mechanisms for mast cell-dependent urticaria are included in Table 18.1 . Cross-linking of the Fab portion of specific IgE on mast cells by percutaneous or circulating allergen undoubtedly accounts for some cases of acute or episodic urticaria (see Fig. 18.3 ), but this is probably never the cause of adult chronic continuous urticaria. Examples of the former would be contact urticaria from natural rubber latex and acute urticaria from foods, including nuts, fish, and fruit. However, the majority of acute urticaria cases do not relate to allergen exposure.
| ETIOLOGIES AND PATHOMECHANISMS OF WHEALS AND/OR ANGIOEDEMA |
|---|
| Idiopathic |
| Immunologic |
|
| Non-immunologic |
|
IgE has been implicated in the pathogenesis of symptomatic dermographism, cold urticaria and solar urticaria, but the mechanism by which it renders skin mast cells more sensitive to physical stimulation is not certain. It is proposed that the physical stimulus in these patients induces a neoantigen that reacts with specific IgE antibody bound to mast cells. An additional mechanism, such as neuropeptide release, could initiate or potentiate mast cell activation. Using electron microscopy, localized platelet clumping has been demonstrated in cold urticaria, and the release of platelet mediators, including platelet-activating factor (PAF) and platelet factor 4/CXCL4, could contribute to wheal formation.
Cholinergic urticaria develops in response to stimulation of cholinergic sympathetic innervation of the sweat glands. How release of acetylcholine from the nerve endings leads to mast cell activation and histamine release is unknown. An allergy to sweat has been demonstrated by one group of investigators . It has been proposed that pressure-induced wheals may be due to a late-phase reaction, but an antigen has never been identified. In three Lebanese families with autosomal dominant vibratory urticaria, a missense gain-of-function variant was detected in ADGRE2 which encodes adhesion G protein-coupled receptor E2. This was thought to lead to destabilization of the inhibitory interaction between the alpha and beta subunits of ADGRE2, leading to sensitization of mast cells to vibration-induced degranulation .
The initiating event for spontaneous urticaria wheals is unclear but may involve plasma leakage due to local factors such as heat or pressure, which allows the extravasation of autoantibodies or IgE-directed antigens that then activate the IgE receptor, thus leading to mast cell degranulation and a subsequent urticarial response. As functional autoantibodies cannot be detected in ~70% of chronic urticaria sera by currently available tests, other mechanisms may operate in “non-autoantibody” urticaria, which, nevertheless, has a similar clinical presentation . Increased plasma levels of prothrombin fragment 1 + 2 (F 1 + 2) and D-dimer (a measure of fibrinolysis) have been demonstrated in CSU and relate to disease severity, but the contribution of coagulation abnormalities to the pathogenesis remains unclear. There are other serum factors in CSU patients that can activate mast cell lines in vitro and lead to endothelial activation, independent of IgE receptors on mast cells and the presence of IgG .
A popular hypothesis is that dietary food additives and natural salicylates as well as nonsteroidal anti-inflammatory drugs (NSAIDs) may cause urticaria via the diversion of arachidonic acid metabolism from prostaglandin to leukotriene formation. How this leads to urticaria is not clear, but it is known that intradermal injections of LTC 4 , LTD 4 , and LTE 4 cause whealing by a direct action on small blood vessels. There is some evidence from studies of rat peritoneal mast cells that PGE 2 can have inhibitory effects on immunologic mast cell degranulation , so a reduction in their formation may facilitate the latter. Aspirin can aggravate urticaria in up to 30% of patients with chronic disease , and while some clinical studies of dietary pseudoallergen avoidance have given encouraging results, the proportion of complete responders confirmed by rechallenge is small . Aspirin allergy as a cause of urticaria is much less common, and the proportion of patients with urticaria due solely to pseudoallergens is probably low.
Understanding “idiopathic” urticaria remains an important challenge. From a clinical perspective, it should be regarded as a multifactorial problem, and searching for aggravating factors is just as important as looking for causes.
Mast cell-independent urticaria
There are several recognized circumstances where angioedema or wheals are due to mechanisms that do not involve mast cells. These need special consideration because their management and prognosis are different. For example, prostaglandins are involved in the pathogenesis of some patterns of non-immunologic contact urticaria (e.g. to benzoic acid), and the latter can be suppressed by NSAIDs . In the cryopyrin-associated periodic syndromes (CAPS; see below), patients often develop urticarial lesions. Systemic symptoms, such as fever, help to distinguish patients with autoinflammatory syndromes from those with CSU (see Ch. 45 ). The significant improvement that results from the administration of anakinra , an IL-1 receptor antagonist , rilonacept , a fusion protein that contains the extracellular domain of the IL-1 receptor and functions as an IL-1 trap , or canakinumab , a human anti-IL-1β monoclonal antibody , points to the role of the cryopyrin inflammasome and its production of IL-1β (see Figs 4.2 and 45.13 ).
C1 esterase inhibitor (C1 inh) deficiency
C1 inh deficiency is usually hereditary, but may be acquired. Three types of hereditary angioedema (HAE) are now recognized (see Fig. 18.19 ). Types I and II are caused by mutations in one allele of the structural gene for C1 inh, resulting in reduced levels of C1 inh (85% of cases; type I) or reduced C1 inh function (15% of cases; type II). Because the mutations lead to levels that are 5–30% of normal (rather than the expected 50%) in patients with type I HAE, it is thought that there is trans inhibition of the normal allele or increased catabolism of C1 inh.
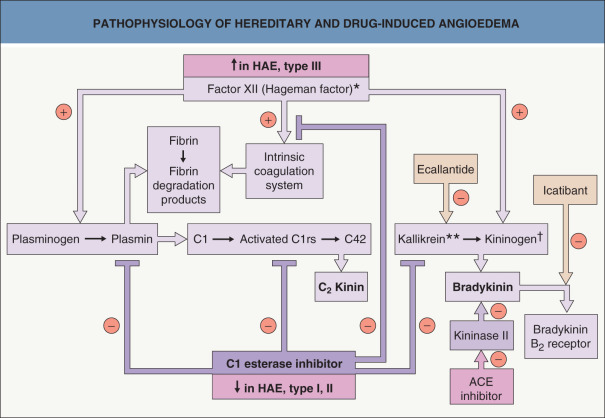
Deficiency of C1 inh leads to loss of inhibition of factor XII (FXII; Hageman factor), resulting in the generation of bradykinin by the action of kallikrein on high-molecular-weight kininogen ( Fig. 18.6 ). Activation of the C1 component of complement by proteolytic enzymes, including plasmin and FXIIa, leads to low levels of C4 in the serum, which is an almost constant feature between and during attacks in untreated patients. Of note, HAE with normal C1 inh activity, also known as type III HAE , may be due to an activating mutation in one allele of the gene that encodes FXII, leading to increased formation of bradykinin. One possible explanation for the preponderance of women is the enhancement of transcription of this gene by estrogens. In addition, there is a positive feedback loop between kallikrein and FXII.
Acquired deficiency of C1 inh may result from activation of C1q and the complement cascade in patients with B-cell lymphoproliferative disorders and plasma cell dyscrasias, or in those with autoimmune connective tissue diseases. This leads to consumption of C1 inh plus low serum levels of C1q as well as C4 (acquired, type I) or the formation of inhibitory autoantibodies directed against the C1 inh (acquired, type II).
Angiotensin-converting enzyme (ACE) inhibitor-induced urticaria is believed to result from the inhibition of endogenous kininase II (also known as ACE), which leads to increased production of bradykinin via inhibition of its metabolism (see Fig. 18.6 ). It usually presents with angioedema, which is usually orofacial and may be life-threatening.
Clinical Features
Clinical Diversity
It is important to distinguish urticaria from urticarial dermatoses , such as urticarial drug eruptions, eosinophilic cellulitis, and the urticarial phase of pemphigoid. The individual wheals of urticaria are “here today and gone tomorrow” (i.e. they generally last <24 hours), whereas with urticarial dermatoses, the individual lesions last for days or longer. Although urticarial vasculitis is often included in classifications of urticaria because the wheals resemble urticaria, it is actually an urticarial dermatosis. Clinically, the lesions last longer than 24 hours (as determined by circling and observing individual wheals), and histologically there is evidence of leukocytoclastic vasculitis (see Ch. 24 ).
Wheals may be small or large, as well as single or multiple. In the physical urticarias, the distribution pattern and morphology can be helpful in separating the different clinical types (see Physical Urticarias ). Angioedema can merge with wheals and these two can be difficult to separate, especially around the eyelids. Angioedema may also be a feature of anaphylaxis, if the throat is involved. In this sense, wheals, angioedema, and anaphylaxis form parts of a clinical spectrum.
Classification
Because the etiology is often unknown at the time of the first consultation, the most practical classification of urticaria relies on clinical characteristics rather than etiology when defining groups of patients ( Table 18.2 ). Most spontaneous urticaria can be considered to behave in an ordinary manner (i.e. fluctuating wheals which may be accompanied by angioedema) whatever its etiology or duration, unless it has a predominantly physical trigger, has evidence of vasculitis, or is caused by exogenous contact. If no cause for spontaneous urticaria can be defined, it is called idiopathic, but the use of this label as an automatic prefix to chronic urticaria is no longer tenable as a significant number of these patients will have an autoimmune etiology. It is worth separating angioedema without wheals from the other patterns of urticaria, because some of these cases will be due to HAE, acquired C1 inh deficiency, or drug reactions (e.g. ACE inhibitors, NSAIDs), and these are managed differently.
| URTICARIA – CLINICAL CLASSIFICATION AND DIFFERENTIAL DIAGNOSIS |
|---|
| Clinical classification |
|
| Differential diagnosis |
|
* Included within the inducible urticarias in the EAACI/GA 2 LEN/EDF/WAO Guideline .
Acute Versus Chronic Urticaria
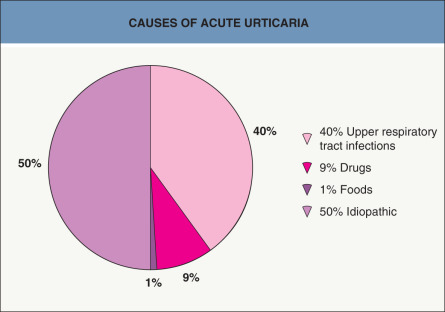
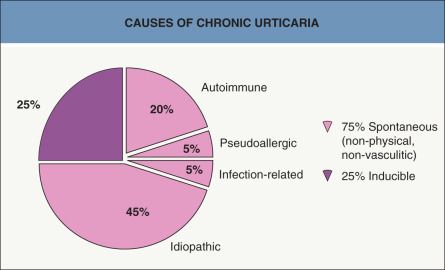
All urticarias are acute initially. Some will become chronic after a period of time that is usually defined as 6 weeks or more. The term “chronic urticaria” should only be applied to continuous urticaria occurring at least twice a week off treatment. Urticaria occurring less frequently than this over a long period is better called episodic (or recurrent), because this presentation may be more likely to have an identifiable environmental cause. The causes of acute urticaria presenting to emergency dermatology clinics in one survey are shown in Fig. 18.7 . Most of these patients probably fall into the spontaneous category, because physical urticarias and urticarial vasculitis tend to persist beyond 6 weeks and contact urticarias would not normally present to the hospital. The high frequency of associated viral infections is notable, as is the lack of food allergy as a cause. The different clinical patterns of chronic urticaria and their causes (where known) are shown in Fig. 18.8 . These data reflect the experience of specialist urticaria clinics in dermatology departments and may not represent the experience of other medical practitioners, such as those in general practice, internal medicine, pediatrics, or allergy.
Spontaneous Urticaria
The condition can present at any age. Acute urticaria is common in young children with atopic dermatitis, but chronic urticaria peaks in the fourth decade. Multiple pruritic wheals of different sizes erupt anywhere on the body and then fade within 2–24 hours without bruising; angioedema may last up to 72 hours when severe. Wheals may occur at any time, but often appear in the evening or are present on waking. Irritation tends to be most intense at night and may disturb or prevent sleep. This, in turn, compounds the distress of the condition. Substantial impairment in quality-of-life measures, including self-image, sexual relationships and social interactions, has been demonstrated. Women may describe premenstrual exacerbations. Systemic symptoms of fatigue, lassitude, sweats and chills, indigestion, myalgia or arthralgia may occur with severe attacks, but the occurrence of pyrexia or arthritis should alert the clinician to another explanation, such as urticarial vasculitis, Schnitzler syndrome, or cryopyrin-associated periodic syndrome (e.g. Muckle–Wells syndrome).
Associations
Chronic spontaneous urticaria has been associated with autoimmune thyroid disease and other autoimmune conditions, including vitiligo, insulin-dependent diabetes, rheumatoid arthritis, and pernicious anemia . Those chronic urticaria patients with demonstrable histamine-releasing autoantibodies have a very strong association with HLA DRB1*04 (DR4) and its associated allele DQB1*0302 (DQ8) . A possible association between Helicobacter pylori gastritis and chronic urticaria was suggested by a systematic review of therapeutic studies, which showed a higher frequency of urticaria remission when the infection was eradicated than when it was not . Parasitic infections, such as intestinal strongyloidiasis, are an uncommon cause of urticaria in developed countries, but may be a significant problem where they are endemic. Acute urticaria due to gastric Anisakis simplex has been reported from Spain . Possible associations between dental infections or gastrointestinal candidiasis and chronic urticaria have not been substantiated by large epidemiologic studies. Although there have been anecdotal reports linking urticaria to malignancy, no statistically significant association was found in a Swedish survey . However, an increased risk of hematologic malignancies, especially non-Hodgkin lymphoma, was noted in a large retrospective cohort study of a National Insurance database in Taiwan .
Inducible Urticarias (syn. Physical Urticarias)
These urticarias represent a distinct subgroup of the urticarias that is induced by an exogenous stimulus rather than occurring spontaneously. Because cholinergic urticaria is triggered by factors that lead to sweating (e.g. a rise in core body temperature, stress, spicy foods), rather than an external physical stimulus, it is often classified separately from other inducible urticarias. The inducible urticarias are classified by the predominant stimulus that triggers whealing, angioedema, or anaphylaxis ( Table 18.3 ). Of all the urticarias, they may affect the quality of life most severely, particularly delayed pressure urticaria and cholinergic urticaria . While the lesions of most physical urticarias occur within minutes of provocation and generally resolve within 2 hours, a few physical urticarias (e.g. delayed pressure urticaria, delayed dermographism) develop after a delay of several hours and persist for 24 hours or longer.
| CLASSIFICATION OF INDUCIBLE URTICARIAS |
|---|
| Urticaria due to mechanical stimuli |
Dermographism
Delayed pressure urticaria Vibratory angioedema
|
| Urticaria due to temperature changes |
Heat
Cold
|
| Urticaria due to sweating or stress |
| Cholinergic urticaria Adrenergic urticaria Exercise-induced urticaria
|
| Contact urticaria |
| Solar urticaria |
| Aquagenic urticaria |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


