Chapter 5
Urticaria and Angio-oedema
OVERVIEW
- Definition and pathophysiology; the role of vasodilators.
- Classification.
- Clinical presentation of different types of urticaria.
- Causes and investigation of non-physical urticarias.
- Management and treatment.
Introduction
Urticaria describes transient pruritic swellings of the skin, often referred to as wheals, hives or nettle rash by the patient. Urticaria results from oedema in the superficial layers of the skin causing well-demarcated erythematous lesions. It may be associated with allergic reactions, infections or physical stimuli, but in most patients no cause can be found. Similar lesions may precede or be associated with vasculitis (urticarial vasculitis), pemphigoid or dermatitis herpetiformis.
Angio-oedema in contrast is usually painful rather than itchy and appears as a diffuse swelling that affects the deeper layers of the skin; it can occur rapidly and may involve the mucous membranes. Laryngeal oedema is the most serious complication and can be life threatening. Hereditary angio-oedema is a rare form with recurrent severe episodes of subcutaneous oedema, swelling of the mucous membranes and systemic symptoms.
Urticaria is a common skin disorder that affects 20% of the population at some point in their lives. Urticaria may occur as a single episode or be chronically recurrent. It is often self-limiting and is controlled with over-the-counter antihistamine. The prognosis is varied depending on the underlying cause, but in chronic idiopathic urticaria symptoms may persist for several years.
Pathophysiology
Urticaria results from histamine, bradykinin and proinflammatory mediators being released from basophils and mast cells in response to various trigger factors. The chemicals released by degranulation cause capillaries and venules to leak causing tissue oedema. Urticaria may be IgE mediated with cross-linking of two adjacent IgE receptors, or complement mediated (causing direct degranulation of mast cells), or mast cells may be directly stimulated by an exogenous or unknown substance. In patients with chronic urticaria, histamine can be released spontaneously or in response to non-specific stimuli and their vasculature is more sensitive to histamines.
Clinical history
Careful history-taking is of great importance in diagnosing patients with urticaria and/or angio-oedema because frequently there are no clinical signs for the medical practitioner to see. Ask about the onset, duration and course of lesions, rashes and swelling. Urticaria is very itchy and angio-oedema usually painful. Patients with urticaria complain of itchy spots or rashes lasting minutes or hours (usually less than 24 h) that resolve leaving no marks on the skin. Patients may complain of swelling (angio-oedema) of their face, particularly eyelids, lips and tongue, which may last hours or days.
If the skin eruption lasts for more than 24 h, is painful and resolves with bruising then urticarial vasculitis (Figure 5.1) is more likely than ordinary urticaria (Figure 5.2).

Figure 5.1 Urticarial vasculitis with bruising.

Figure 5.2 Ordinary urticaria.
Patients may feel unwell before the onset of the rash or swelling and rarely in severe reactions anaphylaxis can occur. You should always ask about any associated respiratory distress. An attempt to identify possible triggers before the onset of symptoms is important. In particular, ask about any food eaten (nausea/vomiting), exercise, heat/cold, sun, medications/infusions, latex exposure, insect stings, animal contact, physical stimuli, infections, family history and any known medical conditions (Figures 5.3 and 5.4).

Figure 5.3 Urticaria from contact with brown caterpillar moths.
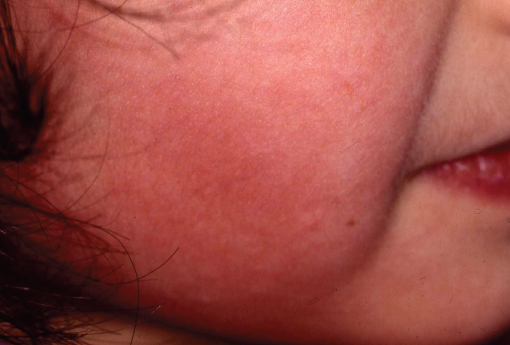
Figure 5.4 Cold-induced urticaria on the cheeks.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


