Chapter 17
Insect Bites and Infestations
OVERVIEW
- Bites can cause a local skin reaction and/or systemic disease in humans through the transmission of parasites, bacteria or viruses.
- Biting insects (including mosquitoes, midges, bedbugs, fleas, sandflies, mites, ticks and lice) cause erythematous pruritic lesions on exposed skin, usually in groups/clusters.
- A generalised anaphylactic reaction to an insect sting can be life threatening. Patients known to be at risk should carry a preloaded syringe of adrenaline to use when reactions occur.
- Worldwide, scabies is the most common infestation. Female mites burrow through the skin, resulting in intense itching.
- Other infestations include lice (which may transmit trench fever and typhus). Pubic lice may be associated with other sexually transmitted diseases.
- Cutaneous larva migrans occurs when larvae from the dog/cat hookworm penetrate human skin, causing a superficial creeping eruption.
Insect bites and stings
When insects bite, they inject their saliva into the skin and ingest blood, which usually causes localised areas of discomfort and itching (Figure 17.1), which may be clustered or in a linear distribution (Figure 17.2). Stinging insects inject venom through the sting that causes a more severe local reaction. More serious effects are due to (a) anaphylactic reactions from the bite/sting or (b) the introduction of infectious diseases.

Figure 17.1 Papular and inflammatory insect bite reactions.
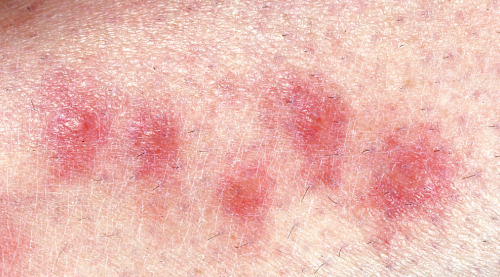
Figure 17.2 Linearity of insect bite reactions.
Most cases of bites from fleas, midges and mosquitoes are readily recognised (Box 17.1) and cause few symptoms apart from discomfort/itching. Occasionally, an allergic reaction confuses the picture, such as large bullae (Figure 17.3). Persuading patients that their recurrent itchy spots are due to flea bites can be difficult and they may reject the suggestion (Box 17.2). Some patients develop a persistent insect bite reaction which lasts for many months (Figure 17.4).

Figure 17.3 Bulla bite reaction.

Figure 17.4 Persistent insect bite reaction.
Box 17.1 Clinical features of bites
- Exposed skin sites, especially lower limbs
- Clustering or linear groups of lesions
- Papules, nodules, urticated lesions
- Blisters or ulceration
- Excoriations with secondary bacterial infection.
Delusions of parasitosis
Patients are convinced they have an infestation with parasites when they do not; the term pseudoparasitic dysesthesia may helpfully be used with patients. Those affected often bring samples in jars of ‘insects’ (Figure 17.5). Examination shows these to be pickings of keratin, cotton or thread. Sympathy and tact should help reassure the patient and help build confidence; derision and disbelief will tend to trigger seeking a second opinion elsewhere. Two thirds of patients have the unshakable belief that they are infested with parasite. Application of topical creams and bandaging may help heal the affected excoriated skin; however, antipsychotic drugs are usually required to treat the psychosis and should be prescribed in conjunction with advice from a psychiatrist. Drugs such as risperidone can be of benefit but care must be taken because of potential side effects, particularly if the patient has epilepsy or cardiovascular disease. More recently, aripiprazole (15 mg for 8 weeks and then 7.5 mg/day) has been shown to be effective. Antidepressants including citalopram have also shown benefit especially in those with concomitant depression.
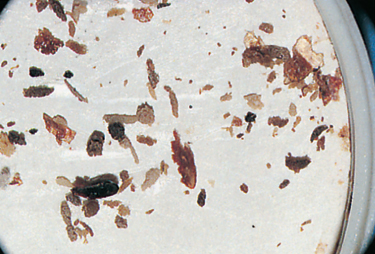
Figure 17.5 Parasitophobia specimens.
Box 17.2 Risk factors for bites
- Outdoor activities
- Travel
- Poor-quality accommodation
- Contact with animals
- Recent death of a family pet.
Allergic reaction to bites
Commonly, insect bite reactions cause local irritation, and rarely (often to stings rather than bites) a generalised anaphylactic reaction may occur. For localised allergic reactions oral antihistamines and topical steroids are effective and for more generalised reactions oral antihistamine, intramuscular (IM) adrenaline (injected into the lateral thigh) and systemic steroids may be required. In those identified as having severe reactions to stings they should be given a self-injectable epinephrine pen to use in subsequent severe reactions.
Management of bite reactions
- Over-the-counter preparations can be used in the majority of cases, such as bite-soothing spray, lidocaine and hydrocortisone ointment.
- Antihistamine creams (crotamiton and doxepin) or tablets (cetirizine and desloratadine) can help reduce itching.
- If blisters are present they can be deflated with a sterile needle.
- Topical steroids such as Betnovate ointment twice daily can be applied to reduce inflammation, swelling and itching.
- If bite reactions are secondarily infected, topical or oral antibiotics may be needed. Topical fucidin ointment or Fucibet cream (a combination steroid and antibiotic) can be used twice daily. Flucloxacillin usually covers secondary staphylococcal infections (erythromycin in penicillin-sensitive patients).
- In very severe cases, a short course of oral prednisolone may be needed (30 mg daily for 5 days).
- If blisters are present they can be deflated with a sterile needle.
Prevention of bites
Keep the skin covered with clothing (especially dark colours), wear insect repellent (WHO recommends Icaridin (Autan®, chemical KBR 3023) and DEET (N,N-diethyl-meta-toluamide)) and sleeping under bed nets off the ground.
Insect bites transmitting parasites
The identity of the biting insect can be important information if a parasitic infection is suspected. Insects that bite humans include mosquitoes, midges, bed bugs, fleas, sand flies, mites, ticks and lice. Each insect has its own specific distribution, preferred location, seasonal activity and preferred skin sites. All these factors can help pinpoint the offending insect (see Table 17.1
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


