| Reconstruction of large (>80%) full thickness defects of the upper eyelid |
| Size and dimensions of upper eyelid defect |
| Involvement of lacrimal system |
| Eyelid laxity |
| Evaluation of donor sites for grafts (contralateral upper eyelid, ipsilateral lower lid, pre/retroauricular, supraclavicular, inner arm) |
| History of prior eyelid, facial surgery or trauma |
| Visual function of both eyes (monocular status) |
| History of smoking/tobacco use |
Introduction
Total defects of the upper eyelid are often the most challenging to reconstruct. Compared to the lower eyelid, the upper eyelid has greater vertical excursion, function and dynamic movement. Ideally, the reconstructed upper eyelid should share a similar purpose with optimum aesthetic appearance.
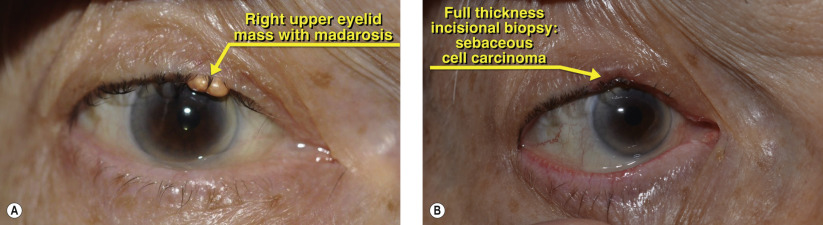
Complete loss of the upper eyelid can occur due to cutaneous malignancy, trauma or developmental anomalies. In reconstruction of larger defects, the bi-lamellar architecture of the eyelid typically requires a combination of flaps and grafts for the most ideal result. Time-honored grafting principles apply in that either the anterior or posterior lamella must provide the vascular supply. Free grafts can be layered on a pedicle-based flap. If the lacrimal system is involved, canalicular reconstruction should be performed primarily but creation of a nasolacrimal conduit should be deferred in cases of tumor.
Smaller defects of the upper eyelid can be closed using a variety of techniques. Direct closure ( Chapter 37 ) and the Tenzel semicircular flap ( Chapter 39 ) work well as non-lid-sharing techniques, but greater sized defects may require pedicle-based grafts from the lower eyelid. Direct closure and the semicircular flap have the advantage of preserving some eyelashes. The Cutler-Beard procedure was originally described in 1955 for reconstruction of large upper eyelid defects. The procedure involves advancing a full thickness (from skin to conjunctiva) myocutaneous flap from the lower eyelid harvested inferior to the inferior tarsal border. The flap is then transferred posteriorly to the preserved lower eyelid margin segment to reconstruct the upper eyelid. Because there is no tarsus present in the advancement flap, a free posterior lamellar graft is typically harvested and placed first in the upper eyelid defect. Choices for posterior lamellar grafts include free tarsal grafts, nasal chondral mucosa and hard palate. A posterior lamellar graft can be omitted but the upper eyelid may be less stable.
As an eyelid sharing procedure, the Cutler-Beard flap needs to gain vascularity prior to the staged release of the pedicle. Ideally this should occur from 4 to 6 weeks after stage one. In monocular patients and in children, eyelid-sharing techniques should be used cautiously due to the interference with vision and possible amblyopia.
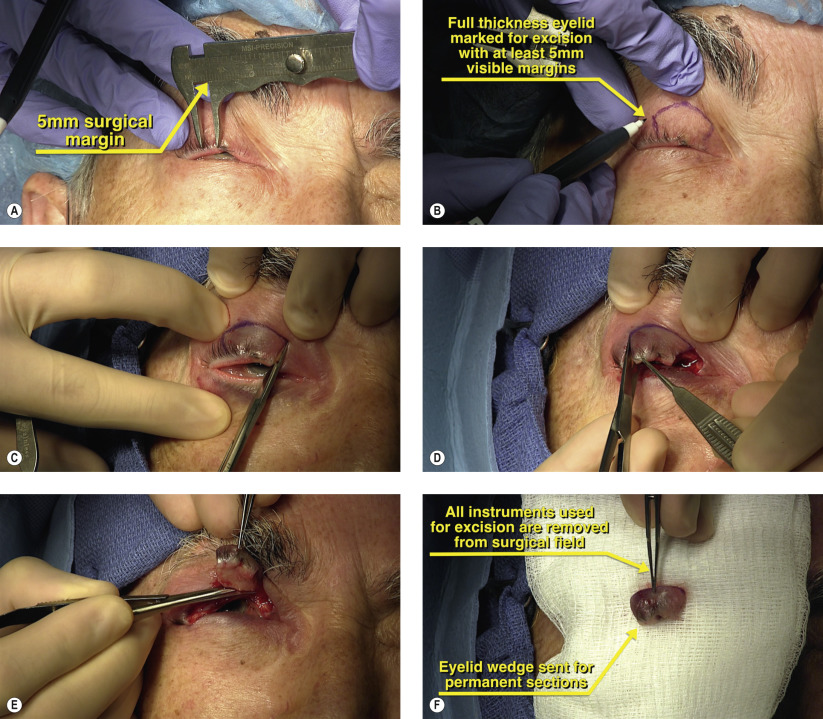
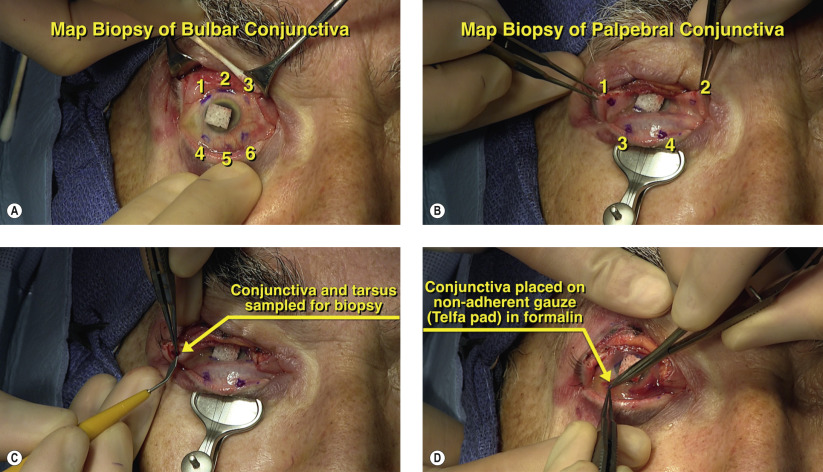
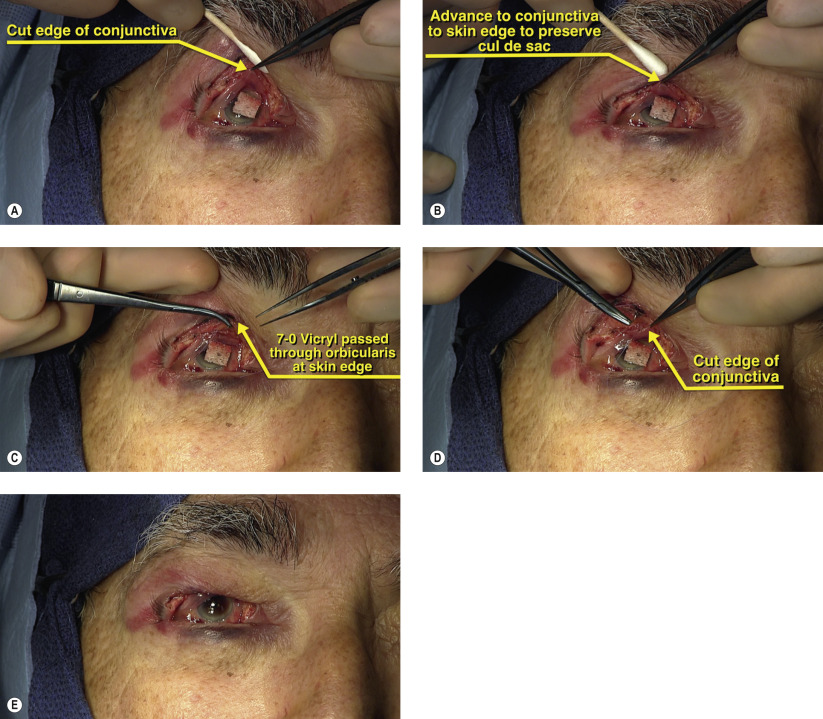
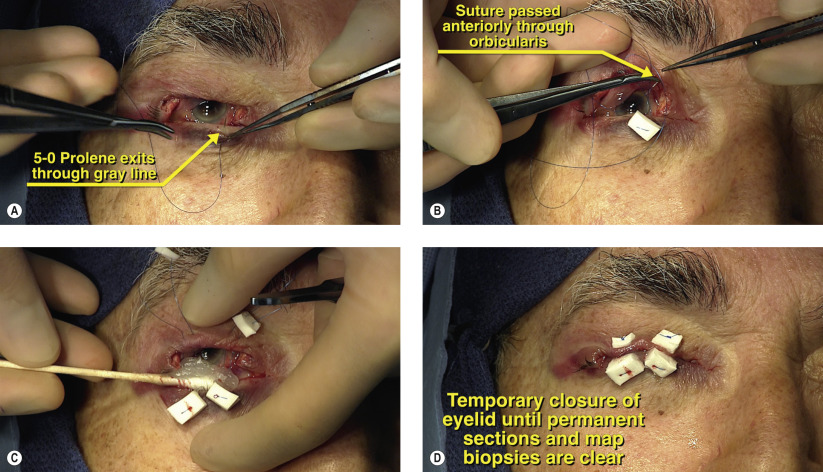
Surgical Technique