| Functional dermatochalasis affecting vision |
| Cosmetically displeasing dermatochalasis and/or upper eyelid fullness |
| To correct associated lash ptosis, entropion, blepharitis or anophthalmic prosthetic instability |
| Use of upper eyelid dermatochalasis for anterior lamellar skin grafting elsewhere |
| Prior facial surgery or trauma |
| Dry eye symptoms |
| Prior refractive surgery |
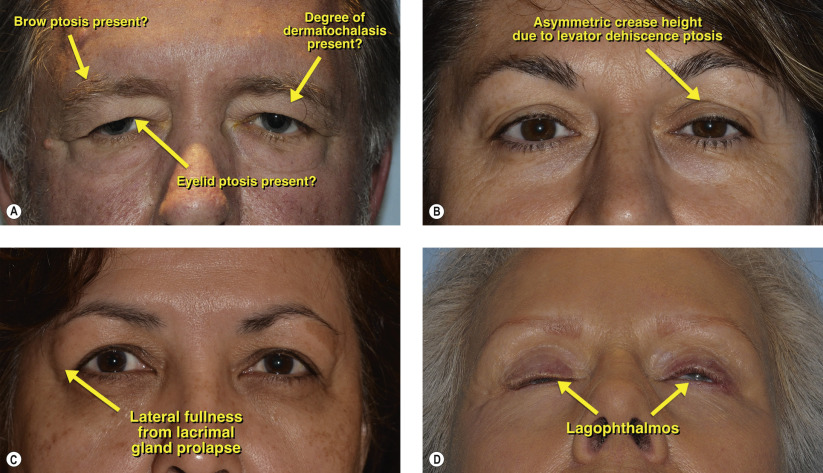
| Degree of dermatochalasis and fat prolapse |
| Presence of lacrimal gland prolapse |
| Presence of concurrent eyebrow ptosis and eyelid ptosis |
| Ethnic differences between Asian and Occidental eyelid crease |
Introduction
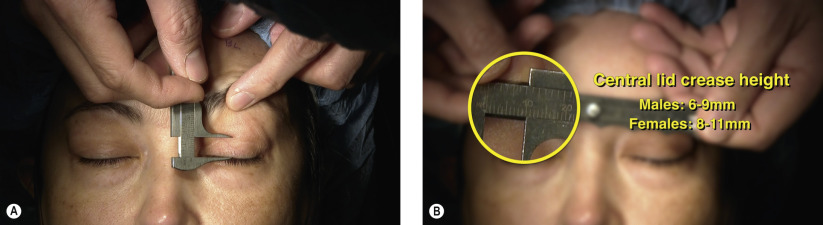
Several parameters should be evaluated in the preoperative blepharoplasty examination. Documentation of functional symptoms, photographs, and visual-field testing are mandatory for coverage by many third-party carriers. When photographing the patient, images should be captured in the frontal plane, three-quarter profile, and the side plane. Before and after photographs documenting improvement and changes are essential particularly for the discerning cosmetic patient. History of dry eye symptoms, prior facial surgery or trauma and refractive surgery are elicited. Aesthetic considerations should be addressed with the patient holding a mirror during the examination to point out salient features. During the examination, the degree of dermatochalasis present should be noted as well as any co-existent brow and/or eyelid ptosis ( Figure 3.1A ). The eyelid creases are then measured for symmetry. Asymmetric eyelid creases are often associated with eyelid ptosis ( Chapter 11 , Chapter 12 , Chapter 13 ) and this should be identified and addressed at the time of blepharoplasty. Often, the higher eyelid crease is associated with levator dehiscence ptosis ( Figure 3.1B ). Lateral eyelid fullness should be noted and palpation may reveal a prolapsed or pathologically enlarged lacrimal gland ( Figure 3.1C ) and require repositing and possible biopsy ( Chapter 70 ). Examination of the tear film (tear breakup time, tear lake, Schirmer’s testing) should be performed as well as assessment for lagophthalmos with the eyelids gently closed ( Figure 3.1D ).
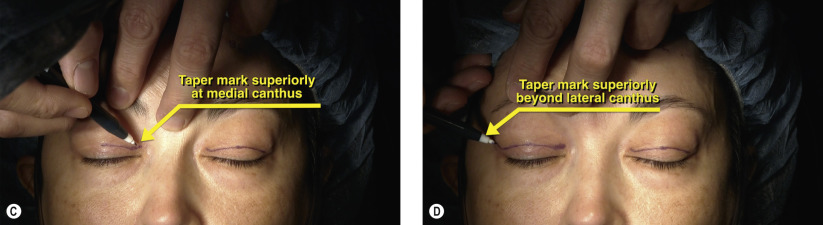
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


