Unilateral Cleft Lip Repair: Millard/Mohler Modifications
Roberto L. Flores
Gerald J. Cho
DEFINITION
A unilateral cleft lip is a congenital separation of the upper lip. The degree of clefting can be microform, minor form, incomplete, or complete.
Microform
Discontinuity of the vermilion-cutaneous junction
Cupid’s bow symmetrical
Slight notching of mucosal free border
Variable nostril deformity and alveolar defect
Minor form
Vermilion notch greater than 3 mm above the level of Cupid’s bow on the noncleft side
Discontinuity of orbicularis oris
Nasal deformity
Alveolar cleft present
Incomplete
Complete full-thickness separation of upper lip with intact nasal sill or a Simonart band along the nasal floor
Complete
Complete full-thickness separation of upper lip
ANATOMY
Both the soft (upper lip and nose) and hard tissues (maxilla, septum, lower lateral cartilages of nose) are affected (FIG 1).
Upper lip—The deformities in this area can be categorized into those affecting the medial and lateral lip elements.
In the medial lip element, Cupid’s bow is preserved but with vertical deficiency of the vermilion. The columella and philtral column are shortened on the cleft side. The orbicularis oris has an abnormal and unilateral insertion at the nasal base, and its disruption results in vertical shortening of the medial upper lip, superior rotation of the Cupids bow, and vertical shortening of the vermilion.
In the lateral lip element, the height and transverse length are shortened. Medially, there is a distinct point where the white cutaneous roll and junction of the wet and dry vermilion start to converge medially (Nordhoff point). The pars superficialis on the lateral lip alters the direction of this muscle to run almost vertically in the area below the ala, leading to aberrant attachments to the nostril and periosteum of the piriform aperture. This leads to a vertically foreshortened lateral lip, sometimes producing a bulge in this area.
Nose—The alar base on the cleft side sits on the piriform margin of the maxilla, which is laterally and posteriorly displaced. The malposition of the bony foundation combined with separation of the orbicularis oris causes unopposed action of the ipsilateral zygomaticous major. This results in widening of the nostril, depression of the alar dome, and canting of the columella toward the cleft side (see FIG 1). Unilateral attachment of the orbicularis oris to the medial crura footplates, anterior nasal spine, and caudal septum on the noncleft side exacerbates the columellar tilt and contributes to deviation of the caudal septum toward the noncleft side. Internally, the caudal portion of the ala has a vestibular web. The underlying cartilaginous structures are also malformed. On the cleft side, the medial crus of the lower lateral cartilages is shortened, and the lateral crus is elongated and inferiorly displaced. The septum is dislocated out of the vomer and bows toward the cleft side.
Maxilla—The underlying skeleton forms the platform upon which the soft tissues rest. Thus, the skeletal abnormalities of the maxilla can explain many of the soft tissue abnormalities seen, particularly in the nose. The greater segment of the alveolus is anteriorly rotated due to the fetal protrusion of the tongue. The lesser segment of the alveolus rotates posteriorly. The medial buttress of the maxilla can be hypoplastic and posteriorly displaced.
PATIENT HISTORY AND PHYSICAL FINDINGS
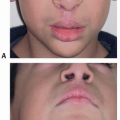
The preoperative assessment of a patient with a unilateral cleft lip includes complete physical exam with assessment for other comorbidities. Facial exam includes the side (left vs right vs midline), the degree of clefting (microform, minor form, incomplete, or complete), and the extent of nasal deformity.
IMAGING
Typically not needed unless within the context of a midline or facial cleft
SURGICAL MANAGEMENT
This surgery is often the first step in the larger multidisciplinary treatment plan for cleft care.
The quality of the primary repair establishes the initial function and appearance for the patient and has great bearing on their future quality of life.
Nasoalveolar molding (NAM) is strongly recommended for patients with a complete cleft or a significant nasal deformity.
Microform clefts can be repaired with less extensive methods than a full rotation advancement.
Minor forms can be repaired with a modified rotation-advancement-type repair with complete primary nasal reconstruction.
Incomplete and complete clefts can be repaired with a full rotation-advancement-type repair.
Initial lip and nose repairs are performed at approximately 3 months of age.
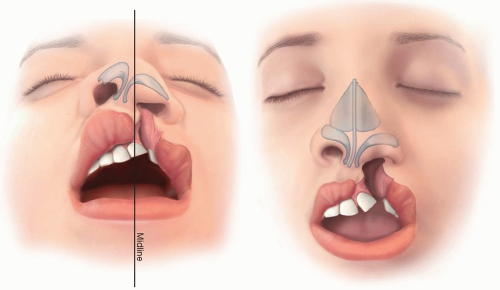 FIG 1 • The soft (upper lip and nose) and hard tissue (maxilla, septum, lower lateral cartilages of nose) anatomy of a left complete unilateral cleft lip. |
Preoperative Planning
The authors use NAM in patients with a complete cleft or a significant nasal deformity. As mentioned above, a cleft through the maxilla not only disrupts the platform upon which the soft tissues sit but also interrupts the dental arch. NAM can help correct the outwardly rotated greater segment and posterolaterally displaced lesser segment. The correction of the skeletal platform into an anatomic position helps place the lip and nose into a more favorable alignment. Furthermore, when the alveolar segments are aligned within 1 mm, a gingivoperiosteoplasty can be performed, which can avoid a secondary bone grafting procedure in 60% to 73% of patients without detriment to midface growth by midterm follow-up. For these reasons, we feel that NAM provides a more predictable lip and nose repair and potentially decreases the overall number of surgical procedures for the child.
NAM typically commences 2 weeks after birth and is completed after 10 weeks of therapy in patients with a unilateral cleft.
Positioning
Supine with gentle neck extension from a shoulder roll
Approach
There are many techniques to repair a unilateral cleft lip, each with its own advantages and disadvantages. In this chapter, we will present Cutting’s modification of the extended Mohler repair.
In this approach, there are eight main steps to the operation: markings, incisions, medial lip dissection, lateral lip dissection, mucosa closure, nasal dissection, lip closure, and nasal refinement.
TECHNIQUES
▪ Millard/Mohler Modifications for Unilateral Cleft Lip Repair
Markings (TECH FIG 1A-D)
Medial and lateral lip elements (TECH FIG 1A)
Medial lip element: The depth (point 1) and height of the noncleft side (point 2) are identified and marked. The distance between these two points is used to mark the height of the Cupid’s bow on the cleft side (point 3). The white roll usually starts to disappear at this point. If Cupid’s bow is wide or indistinct, the marks can be placed more narrowly so that less downward rotation is required.
Lateral lip element:
The height of the lip from the alar base to the height of the Cupid’s bow on the noncleft side is measured with a caliper, and the vertical distance is used to locate the corresponding white roll point on the lateral lip element (point 4). Some surgeons use the widest point of the vermilion (Nordhoff point) to determine point 4. However, in patients with a wide cleft, Nordhoff point will commonly result in a vertically foreshortened lip. Using the vertical height of the contralateral upper lip can sacrifice horizontal lip length for preservation of vertical lip height. The horizontal lip discrepancy will correct over time; however, a vertically shortened upper lip will remain.
Mohler Back Cut (TECH FIG 1B)
The apex of the back cut is critical to the success of the design (see Pearls below). This point (point 5) is placed approximately 1.5 mm superior to the base of the columella and just over halfway (four-sevenths) across the noncleft side.
A line is drawn connecting point 5 to a point just lateral to point 3. This line should be bowed out to the same degree as the philtral column of the unaffected side to recreate the subtle curve.
A straight line is drawn from the apex of the Mohler backcut (point 5) to the height of the philtrum on the noncleft side but no farther (point 6). The angle formed by these two lines and length of the backcut will affect the degree of downward rotation of the Cupid’s bow.
C flap and M flap on the medial lip element (TECH FIG 1C)
C flap: A line is drawn along the skin/mucosa junction lateral to point 3. Care is taken to incorporate as much white lip into the C flap as possible while avoiding the mucosa (see Pearls below).
M flap: The medial/inferior border of the M flap is drawn as a straight line starting from point 3 and perpendicular to the white roll. A second line is drawn on the vermilion of the medial lip element as an oblique line starting at a point 1 mm inferior to the white roll, traveling laterally and inferiorly to the red line. This is the receiving incision for the Nordhoff triangular flap.
Alar base and L flap on the lateral lip element (TECH FIG 1D)
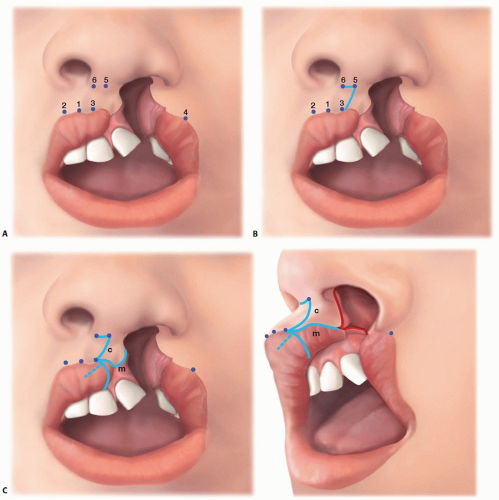
TECH FIG 1 • Markings. A. Key tattoo points. B. Mohler back cut. C. C flap and M flap. Dashed blue line represents the receiving incision for a vermilion triangular flap if used. The dashed red line represents the intranasal incisions on the septum and vomer made during nasal floor closure.
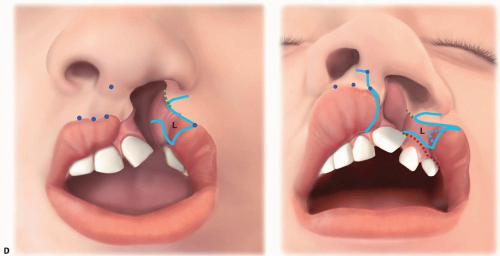
TECH FIG 1 (Continued) • D. Alar base and L flap (L) outlined in blue. The dashed blue line is the triangular flap as described by Nordhoff. Dashed green line is the intranasal incision at the piriform aperture, and the dashed red line is the gingivobuccal sulcus incision, which will be made at the time of the lateral lip dissection.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access