Chapter 29 Umbilicoplasty
Introduction
Abdominoplasty is a very important operation to improve body contour. The first one is credited to Kelly1 in 1899. A previous description of skin and subcutaneous fat tissue resection was performed by Demars and Marx2 in 1890. According to Sinder3 this information was referred to by Voloir4 in his thesis in Paris in 1960. Over many years several abdominoplasty techniques have been described5–7 through different incisions by using a simple procedure of panniculus resection without transposition of the umbilicus. In 1957 Vernon8 described transversal abdominal lipectomy with navel transposition, which is a remarkable step in abdominoplasty.
In his original publication Vernon performed a circular incision around the umbilicus to separate it from the abdominal panniculus flap. Consequently, the surface of the umbilicus was a circle (Fig. 29.1). For its reimplantation, another circular incision and resection was done on the abdominal flap to locate the new navel.
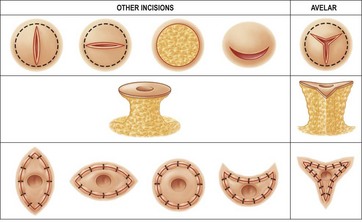
FIG 29.1 APPEARS  ONLINE ONLY
ONLINE ONLY
Concerning the creation of the new umbilical region during abdominoplasty many authors have proposed various types of incisions around the umbilicus itself as well as for its reimplantation on the abdominal wall (Fig. 29.1). The final scar around the transposed umbilicus may be circular.5,6,9–11 Independent of whether the incision on the abdominal flap is vertical, horizontal, circular, or semicircular, because the surface of the umbilicus is a circle the final scars have a tendency to be circular. When my method is adequately performed the final scar is not a circle, but star-shaped around the new umbilical area.
According to a survey by Grazer and Goldwyn12 in 1977, regarding 10 540 abdominoplasties carried out by plastic surgeons from the USA and other countries, umbilical scar contractures may occur in 45% of surgeries. In that survey, they mentioned that 2% of surgeons believe that some sort of retraction or contraction of the umbilical scar always occurs after abdominoplasty when transposition is done. Following my method, the final scar on the umbilicus region after abdominoplasty is not a circle on the surface of the abdominal wall as in the use of other techniques, but a multiple and atypical Z plasty which makes a natural depression of the umbilicus without an external scar.
Preparation, Diagnosis, and Patient Presentation
When I developed and described my method13 in 1976, I used to perform abdominoplasty following the conventional techniques of Callia9 and Pitanguy,6 with wide undermining of the abdominal panniculus from the suprapubic region up to the costal margin. Therefore, my previous publications14–18 were described showing the raw area all over the muscular abdominal structures. However, after the presentations and publications19–22 of my new procedure of abdominoplasty without panniculus undermining (lipoabdominoplasty), I used the same method of umbilicoplasty as previously described. Therefore, since 1999 when I described my technique19 where the abdominal panniculus is not undermined during surgery, all perforator vessels are preserved in order to maintain normal blood supply to the abdominal panniculus. It is important to emphasize the surgical principles of my technique of umbilicoplasty in order to demonstrate the philosophy of the method when the umbilical region is treated during abdominoplasty as well as during treatment of other deformities of the umbilicus:
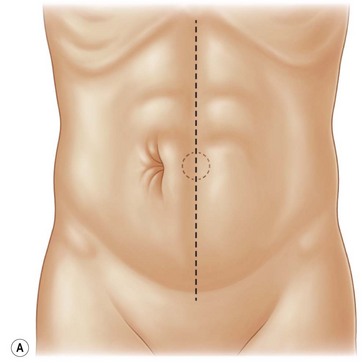
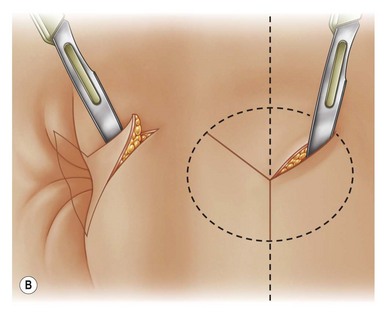
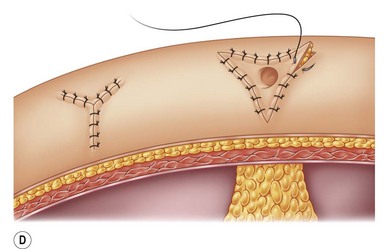
1. Star-shaped incisions are performed around the umbilicus to create three cutaneous flaps on the umbilicus instead of a circular one as is done in other techniques (Fig. 29.2A–F).
2. One of those three flaps is directed downwards and the others are directed upward to the right and to the left.13–15 The main reason for the downwards direction of one flap is to give the postoperative umbilicus a natural inclination to the bottom (Figs 29.3 and 29.4), since this is the normal position of the umbilicus before operation.
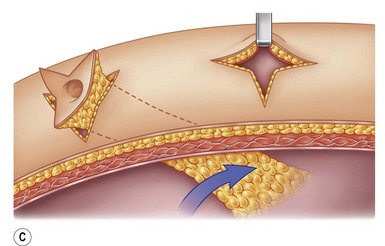
3. Three triangular cutaneous flaps are created on the abdominal wall, which are sutured on the deeper vertices of the umbilicus. This principle means that three cutaneous flaps of the abdominal wall “go” from the surface of the abdominal wall to a deeper point of the umbilicus, making a 90° angle rotation. Such rotation reproduces the similar “migration” of the umbilicus on a newborn child a few days after birth, since the skin around the umbilicus is retracted until it reaches the muscular-aponeurotic wall. In fact, the umbilicus is the first scar in the human body healed secondarily due to its “migration” from outside to the depth.15 Therefore, my method reproduces the natural phenomenon that happens to the umbilicus of a newborn child.
4. Defatting the three cutaneous flaps created on the abdominal wall in order to reduce the thickness of the panniculus around the new umbilical region. This concept is very important, since a normal umbilicus is thinner and gives a depression to the whole umbilical area (Fig. 29.3A–E).
5. Shortening the pedicle of the umbilicus is an important procedure in order to reduce the distance between the abdominal cutaneous flap and the umbilicus itself (Fig. 29.5). This indication is more frequent on patients with obese panniculus as well as on those patients with hernia of the umbilicus with diastasis of the rectus muscles.
6. The final scar around the new umbilical area is a triangular one created by multiple and atypical Z plasty, which avoids scar retraction and contraction postoperatively (Fig. 29.3).

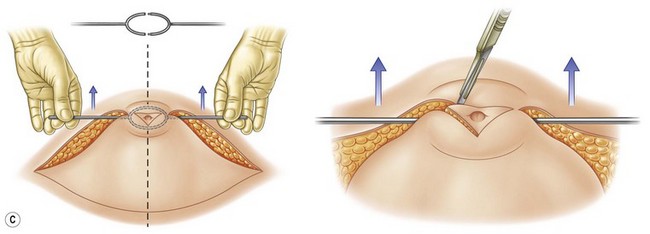
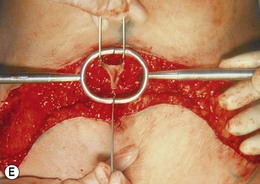
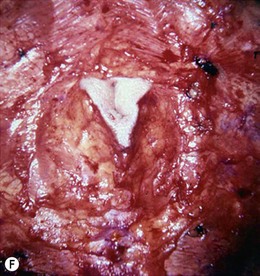
FIG. 29.2 Sequence of schemes and photos showing cutaneous incisions for umbilicoplasty by Avelar’s technique.


FIG. 29.2 Sequence of schemes and photos showing cutaneous incisions for umbilicoplasty by Avelar’s technique.












FIG. 29.4 Placement and transplantation of the umbilicus, before (A, B, C, D) and after (E, F, G, H).
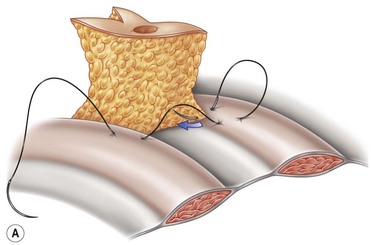
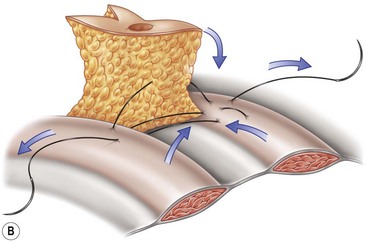
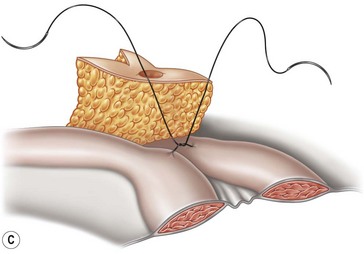
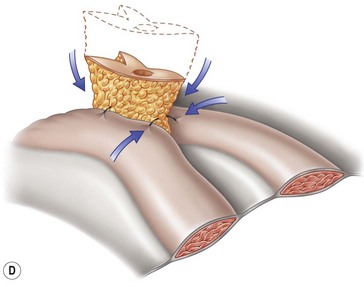
FIG 29.2D, 29.3A–D, 29.4, 29.5 APPEARS  ONLINE ONLY
ONLINE ONLY
Patient Selection
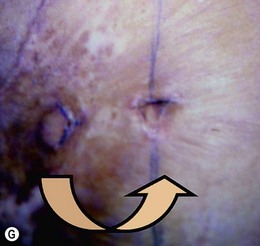
Although my umbilicoplasty method was developed and created during abdominoplasty, I have found several circumstances to use it for treatment and correction of other deformities in the umbilical area. Hernia formation, even with redundancy of skin on the umbilicus, is a very common unesthetic abnormality that may happen in children, leading to an unattractive appearance (Figs 29.6A–G and 29.7A–C). The treatment and correction of those deformities is performed with my method, even with reinforcement of the muscular aponeurosis diastases (Figs 29.6 and 29.7). When children present with diastasis of the rectus abdominalis it is possible to perform reinforcement above and below the umbilicus through the triangular incisions on the umbilicus. Afterwards, if any redundant skin is present it may be resected, leaving the three triangular flaps on the external area of the umbilicus (Figs 29.6 and 29.7).
< div class='tao-gold-member'>







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


