Chapter 74 Tunnel Widening After Anterior Cruciate Ligament Reconstruction
Introduction
Tunnel widening after anterior cruciate ligament reconstruction (ACLR) has been noted for many years. Initially there were concerns that this widening would be progressive. However, it is now clear that tunnel widening only occurs in the first postoperative year1,2 and is not progressive after that period. A number of variables have been hypothesized to cause or contribute to tunnel widening. These include the following:
Specific Factors Associated With Increased Tunnel Widening
Hamstring Versus Bone–Patellar Tendon–Bone Graft
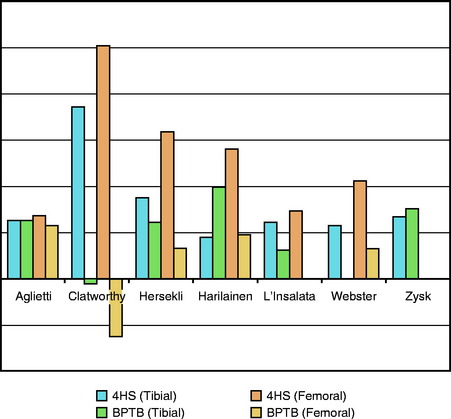
It has been hypothesized that HS grafts are associated with more tunnel widening than BPTB grafts. Tunnel widening has been found with the use of both grafts. Seven series specifically compared HS with BPTB. However, because fixation is different for the HS and BPTB grafts in all these series and because fixation type is one of the leading hypothetical causes of tunnel widening, the isolated effect of graft type is difficult to discern. Of these seven series,2–8 two report tunnel widening that is roughly equal for HS and BPTB and five report more tunnel widening with HS. These seven series are presented in bar graph form in Fig. 74-1.
Allograft Versus Autograft
Two clinical series9,10 have shown increased tunnel widening in allografts versus autografts. In addition, a recent sheep study by Weiler showed increased tunnel widening in allografts at all time periods measured, beginning at 6 weeks and ending at 1 year.11 Possible causes include an increased immunologic response to the graft or the presence of chemical residua in the grafts from processing, cleansing, cryoprotectant, radioprotectant, or the like.
Effects of Fixation Location
It has been suggested that the increased incidence of tunnel widening in HS ACLR may be due to fixation. Specifically, a “windshield wiper” effect resulting in greater tunnel widening when the fixation is further from the joint, as is more often the case with HS than BPTB graft fixation techniques, has been hypothesized. It is theorized that with knee motion, the pressure of the graft on the tunnel wall will vary more with cortical or mid-tunnel (cross-pin) than aperture fixation, producing attrition of the tunnel wall. A review of the literature in this regard does not show a consistent effect of the location of the fixation.12–17 The four studies comparing aperture to cortical or cross-pin fixation are presented in Fig. 74-2.
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


