Key Terms
Squamous Cell Carcinoma in Situ
Bowen disease
Erythroplasia of Queyrat
Keratoacanthoma
Keratoacanthoma centrifugum marginatum
Benign Lichenoid Keratosis
Lichen planus–like keratosis
Tumors with scale are common and represent a heterogeneous group of epithelial neoplasms. This group of important skin tumors includes benign conditions, in situ malignancies (those confined to the epidermis), and frankly invasive cancers. Although the conditions covered in this chapter usually have scale present on the surface, exceptions exist. There may be lesser scale in early or evolving lesions, or, if the tumor is ulcerated, scale may be absent.
Important History Questions
How long has this lesion been present?
The temporal course may suggest a benign or malignant process. A lesion present for years, or even decades, is less likely to be malignant than a lesion that arises quickly, over weeks or months.
Has the lesion recently changed?
Benign lesions can become inflamed (e.g., an inflamed seborrheic keratosis, a lichenoid keratosis arising in a solar lentigo), but a history of evolution sometimes suggests a malignant process.
Is this lesion growing rapidly?
Some malignant processes arise quickly (e.g., keratoacanthoma type of squamous cell carcinoma, aggressive forms of squamous cell carcinoma). Any rapid growth should be noted.
Has the lesion bled?
Any skin lesion, benign or malignant, can bleed when traumatized, particularly if the lesion is exophytic. However, an affirmative response to this question could suggest malignant qualities. A conservative approach is to consider biopsy of any lesion that has bled.
Have you had a previous skin cancer?
Persons with sufficient sun exposure to develop a nonmelanoma skin cancer of any type are at increased risk for a second such neoplasm. Once a person has one nonmelanoma skin cancer, he or she has a 50% chance of having another in the next 3 to 5 years. Skin cancer risk is also affected by chronic immunosuppression, exposure to radiation or arsenic, or infection with oncogenic forms of human papilloma-virus (HPV).
Importan Physical Findings
What is the location of the lesion or lesions?
Certain scaling tumors may be associated with characteristic locations. For example, seborrheic keratoses occur often on the face, chest, and proximal extremities. Squamous cell carcinoma in situ and squamous cell carcinoma occur on sun-damaged skin or the genitalia.
What type of skin does the patient have?
Assessment of patient skin type (Fitzpatrick I–VI) may assist in predicting the risk of kertainocyte derived skin cancer. Persons with fair skin and light eyes are more likely to develop cutaneous malignancies. In particular, persons with red hair and blue eyes are among those at highest risk.
What does the lesion feel like on palpation?
Palpation to identify dermal extension, although imperfect, is useful in differentiating a benign or in situ malignant process from a deeply invasive form of skin cancer.
Squamous Cell Carcinoma in Situ
ICD10 code D04 (one or 2 digits, site dependent)
MALIGNANT NEOPLASIA
Pathogenesis
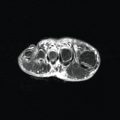
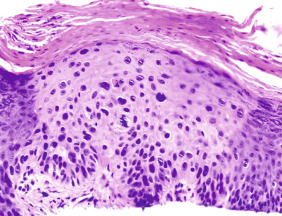
Squamous cell carcinoma in situ (SCCIS), also known as Bowen disease, is intraepidermal form of squamous cell carcinoma. SCCIS can occur on the skin ( Fig. 29.1 ) and mucous membranes. Multiple causative factors are associated with SCCIS, including ultraviolet light, arsenic ingestion, and infection with oncogenic strains of HPV. SCCIS is more common in immunocompromised persons.
Clinical Features
- •
Most SCCIS arises on sun-exposed skin or genitalia of middle-aged to elderly persons.
- •
Patients typically report a persistent lesion, with progressive horizontal expansion. Sometimes, there may be a history of bleeding.
- •
The primary lesion consists of a sharply defined scaly papule or plaque, with variable erosion or ulceration ( Figs. 29.2–29.4 ). There may be inflammation and erythema due to the host response.

Fig. 29.2
Patient with squamous cell carcinoma in situ presenting as a scaly nodule with variable colors, including white, red, and dark purple.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)

Fig. 29.3
Patient with large squamous cell carcinoma in situ presenting as a large scaly plaque between the toes, with marked scale.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)

Fig. 29.4
Patient with human papillomavirus–induced squamous cell carcinoma in situ of the penis. This variant was formerly termed erythroplasia of Queyrat.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)
- •
Some SCCIS may be papillomatous, resembling a wart ( Fig. 29.5 ). Other forms are hyperkeratotic. On occasion, there may even be an overlying cutaneous horn of hyperkeratosis.

Fig. 29.5
Large papillomatous squamous cell carcinoma in situ of the anus that was human papillomavirus–induced in a man who was HIV-positive.
- •
Erythroplasia of Queyrat is a term used for HPV-induced squamous cell carcinoma of the genitalia.
Diagnosis
- •
The history and observation of an expanding scaly and/or eroded papule or plaque on sun-damaged skin is important to the diagnosis. Similarly, an expansive lesion located in the anogenital area is concerning for SCCIS.
- •
The diagnosis must be established by biopsy. A deep shave, large punch (depending on the size of the lesion), or incisional or excisional biopsy may be employed depending on the clinical situation. The latter technique has the potential advantage of providing uninvolved margins, if expressly commented on by the pathologist, thereby providing definitive management.
Treatment
- •
Excision provides for assessment of the surgical margins and exclusion of dermal invasion.
- •
A deep shave biopsy, followed by curettage and electrodessication, is another treatment option. Although this treatment does not require suturing, it precludes margin assessment. Appropriate serial surveillance is necessary to ensure local eradication.
- •
Cryosurgery is less often used, but it does have an adequate cure rate in experienced hands.
- •
Topical 5-fluorouracil may be used, and various products and strengths are available (2% and 5% solutions and 0.5%, 1%, and 5% creams). Typical use is qd or bid for at least 6 to 8 weeks.
- •
Topical imiquimod applied two to three times per week for 16 weeks is an option for some patients.
Clinical Course
SCCIS can grow slowly and insidiously for many years, before later becoming invasive. The risk of progression for SCCIS to frankly invasive squamous cell carcinoma (SCC) is from 5% to 15% per year.
Squamous Cell Carcinoma
ICD10 code C44 (two or three digits, site dependent)
MALIGNANT NEOPLASIA
Pathogenesis
SCC is the second most common skin cancer, second to basal cell carcinoma, with an estimated 200,000 to 700,000 new cases per year. Most SCC is caused by exposure to ultraviolet light (outdoors or in tanning beds), radiation therapy, arsenic ingestion, or some petroleum products. SCC can also occur at sites of chronic injury, including burn scars, chronic skin infections, chronic ulcers, and chronic inflammatory conditions (e.g., lichen sclerosus). Importantly, SCC occurs more often in immunocompromised patients and may behave in an aggressive fashion in this population. Invasive SCC may arise in precursor lesions, such as actinic keratoses (see Fig. 29.5 ), SCCIS (Bowen disease), or within leukoplakia on mucosal surfaces.
Clinical Features
- •
SCC usually occurs on chronically sun-exposed skin of middle-aged or elderly persons.
- •
SCC often presents as a persistent lesion with progressive enlargement, possibly with bleeding.
- •
The clinical presentation is variable, but most often SCC consists of a scaly papule ( Fig. 29.6 ), nodule, or plaque ( Fig. 29.7 ) with variable erosion ( Fig. 29.8 ), hemorrhage, or ulceration ( Fig. 29.9 ). An inflammatory host response, such as surrounding erythema, is often observed.