Key Terms
Verrucae Vulgaris
Myrmecia
Verrucae palmaris
Verrucae plantaris
Warts
Verrucae Plana
Epidermodysplasia verruciformis
Flat warts
Condyloma Acuminatum
Anogenital warts
Venereal warts
Seborrheic Keratosis
Dermatosis papulosa nigra
Inflamed seborrheic keratoses
Melanoacanthoma
Sign of Leser-Trélat
Stucco keratosis
Acrochordon
Fibroepithelial polyps
Skin tags
Soft fibromas
North American Blastomycosis
Gilchrist disease
Verrucous Carcinoma
Ackerman tumor
Buschke-Löwenstein tumor
Epithelioma cuniculatum
Papillomatous and verrucous lesions of the skin include viral infections (e.g., warts, molluscum), deep fungal infections (e.g., blastomycosis), and benign and malignant neoplasms. Papillomas are pedunculated or sessile, chiefly epidermal growths, often with a cauliflower-like appearance. Similarly, the term verrucous, as the name implies, suggests an exophytic lesion, like a wart, often with spirelike, outward projections of the epidermis. The linear presentation of papillomatous lesions has been addressed in Chapter 17 .
Common
- •
Acrochordons
- •
Condyloma acuminatum
- •
Dermatosis papulosa nigra
- •
Papillomatous intradermal nevi
- •
Seborrheic keratosis
- •
Stucco keratosis
- •
Verrucae plana
- •
Verrucae vulgaris
Uncommon
- •
Deep fungal infections
- •
Epidermal nevus
- •
Inflamed linear verrucous epidermal nevus
- •
Verrucous carcinoma
- •
Verrucous incontinentia pigmenti
Important History Questions
When did this lesion(s) develop?
The temporal course is important. Some lesions develop acutely (e.g., condylomata acuminata), whereas others are insidious, but can last for decades (e.g., acrochordons, seborrheic keratoses, verrucous carcinoma). Still yet, other conditions may be congenital in nature (e.g., epidermal nevus).
Has the lesion changed?
Many malignant tumors, such verrucous carcinoma, demonstrate relentless and progressive growth, whereas a benign lesion is more likely to remain stable.
Where have you visited or lived in the past few years?
Some infections, like verrucous cutaneous blastomycosis (see Fig. 28.20 ), are more common in certain geographic areas. Infections may also be acquired from travel to endemic areas.
Important Physical Findings
How many verrucous or papillomatous lesions are present?
Some verrucous and/or papillomatous processes are typically multiple (e.g., acrochordons, condylomata, dermatosis papulosa nigra, seborrheic/stucco keratosis), whereas others are most often solitary (e.g., epidermal nevus, verrucous carcinoma).
What is the distribution of the lesions?
Many verrucous and/or papillomatous processes have characteristic distributions. Acrochordons are often found on flexural surfaces, such as the neck, axilla, and inguinal folds. Condylomata acuminata (genital warts) are usually found in or near the genitalia. Dermatosis papulosa nigricans is found around the eyes and cheeks of persons of color. Verrucous carcinoma is usually found in the oral cavity (Ackerman tumor), anogenital area, or on the feet (epithelioma cuniculatum).
What is the arrangement of the lesions?
Some papillomas may be linear (e.g., epidermal nevus, verruca plana), whereas others are widely distributed.
What is the size of the lesions?
Some papillomas are usually small (e.g., acrochordons, stucco keratosis, verrucae plana), whereas others vary in size (e.g., seborrheic keratoses). Some may be usually large (e.g., epidermal nevus, verrucous carcinoma).
Verrucae Vulgaris
ICD10 code B07.8
VIRAL INFECTION
Pathogenesis
Verrucae (warts) are cutaneous and/or mucocutaneous infections of keratinocytes caused by human papillomavirus (HPV). There are more than 100 subtypes of HPV, with some subtypes affecting characteristic skin locations. In most cases, the infection follows direct inoculation of the skin by HPV, presumably through minor (imperceptible) skin breaks. In the United States, the lifetime risk of developing a clinically-relevant HPV infection has been estimated to be about 80%.
Clinical Features
- •
Verrucae can occur in any age group but are most common in young children.
- •
Verrucae can affect any cutaneous site and, occasionally, mucosal surfaces.
- •
Lesions present as skin-colored verrucous papules or plaques ( Figs. 28.1 and 28.2 ), often with overlying scale, which can disrupt normal skin lines (dermatoglyphs). There may be black dots that represent thrombosed capillaries, and this phenomenon can be called “seed warts” by patients.

Fig. 28.1
Multiple periocular verrucae in a child, always a therapeutic challenge.
(From the William Weston Collection, Aurora, CO.)

Fig. 28.2
Patient with multiple periungual warts. The periungual and subungual regions are particularly challenging to treat.
(From the William Weston Collection, Aurora, CO.)
- •
Verrucae often occur on the hands (verrucae palmaris) or feet (verrucae plantaris; Fig. 28.3 ).

Fig. 28.3
Patient with plantar wart.
(From the Fitzsimons Army Medical Center Collection, Aurora, CO.)
- •
Myrmecia (Greek for “ant”) represent endophytic verrucae caused by HPV1 that occur upon the feet (common) or hands (less common). Myrmecia may be painful.
- •
Destructive modalities may spread a wart in peripheral fashion, causing a so-called “fairy ring” of lesions ( Fig. 28.4 ). Still, these treatment modalities are widely used, and the risk is often tolerated.

Fig. 28.4
Patient with the frustrating fairy ring wart that occurred after cryotherapy. The wart has recurred in the margins of the blister, plus the patient now also has a scar from the therapy.
Diagnosis
- •
The diagnosis is often based chiefly upon the clinical appearance of the lesion.
- •
It can be difficult to distinguish plantar warts from corns and callosities because both cause overlying scale. Lesions may be removed from this overlying keratin with a scalpel blade to examine the base. Plantar warts demonstrate a loss of normal skin lines (dermatoglyphs), whereas corns and callosities retain such markings.
- •
Problematic cases can be sampled by a deep shave and submitted for histologic examination.
Treatment
- •
Over-the-counter treatments are usually based on topical salicylic acid, with or without other additives, such as lactic acid. The response rate is from 40% to 84% (average, 61%). Other topical therapies used include cantharidin (so-called “blister beetle juice”), imiquimod, tretinoin, and 5-fluorouracil.
- •
Liquid nitrogen (LN 2 ) cryotherapy is a destructive therapy often used by health care providers. In published studies, the cure rate of LN 2 is between 26% and 96%. Optimal results are achieved with treatment every 2 to 3 weeks. Plantar warts respond better if excess keratin is pared before LN2 treatment and if two freeze-thaw cycles are employed.
- •
Occlusion with duct tape was widely reported in the lay press a number of years ago. Medical evidence suggests the efficacy of duct tape is highly variable.
- •
Immunotherapy includes topical sensitization with diphencyprone or squaric acid dibutylester or the intralesional injection of Candida antigen.
- •
Systemic therapies for recalcitrant warts include oral cimetidine and oral retinoids. The efficacy of these modalities, particularly cimetidine, is dubious.
- •
Laser therapy is usually performed with a carbon dioxide laser or flashlamp pulsed dye laser. The first is an ablative laser, whereas the latter targets the increased blood supply that is present in verruca.
- •
Intralesional therapies include bleomycin, interferon, and formic acid, but these modalities are usually reserved for the most recalcitrant verruca.
Clinical Course
About 40% to 70% of verrucae resolve spontaneously, usually in about 2 years.
Verrucae Plana
ICD10 code B07.8
VIRAL INFECTION
Pathogenesis
Verrucae plana, also known as flat warts, are usually caused by HPV3. Because of differences in the clinical presentation and management, it is useful to discuss separately verrucae plana.
Clinical Features
- •
Verrucae plana are more common in children and young adults but can affect any age group.
- •
Verrucae plana usually occur on the face and dorsal hands but can also affect the trunk and lower extremities.
- •
Lesions are typically numerous and may number in the hundreds.
- •
The primary lesion is a skin-colored to tan to light brown small papilloma that rarely exceeds 3 mm in diameter ( Figs. 28.5 and 28.6 ).

Fig. 28.5
Patient with numerous small tan papillomas in a perioral distribution of focal coalescence into a small plaque.
(From the William Weston Collection, Aurora, CO.)

Fig. 28.6
Patient with numerous small tan, flat warts that are clinically difficult to distinguish from small seborrheic keratoses.
- •
Lesions may become inflamed, with a red or violaceous color ( Fig. 28.7 ).

Fig. 28.7
Patient with verrucae plana with autoinoculation at a site of a superficial injury. These lesions are violaceous in color due to inflammation.
- •
Lesions may appear in a linear configuration due to autoinoculation (see Fig. 28.7 ).
- •
Variations include a so-called “intermediate wart,” which has features of both a flat and common wart.
- •
Epidermodysplasia verruciformis (EV) is a genetic predisposition to extensive flat warts caused by HPV5, HPV8, HPV14, or HPV17. Lesions of EV may mimic other neoplasms or inflammatory conditions ( Fig. 28.8 ). Lesions of EV have some oncogenic potential, and squamous cell carcinoma can arise in some cases.
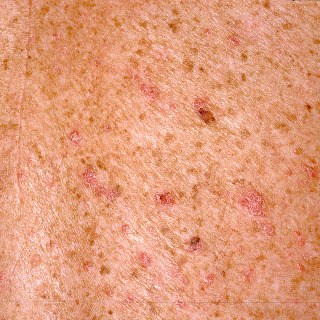
Fig. 28.8
Numerous inflamed red flat papillomas on the trunk in a patient with epidermodysplasia verruciformis.
Diagnosis
- •
In most cases, the occurrence of multiple, small, uniform skin-colored to brownish papillomas is diagnostic. In some cases, it may be difficult to distinguish verrucae plana from other papillomatous conditions, such as seborrheic keratosis.
- •
Problematic cases, including lesions in adults, truncal lesions, and inflamed lesions, should be biopsied to clarify the diagnosis. The findings are often specific (koilocytosis).
Treatment
- •
Verrucae plana can be difficult to treat, and if the lesions are few in number and are not bothersome, therapy is not required. Treating numerous lesions may be challenging.
- •
If treatment is desired, nonscarring modalities, such as topical tretinoin gel (0.025%–0.1% applied qd), is a reasonable option.
- •
Topical imiquimod cream (applied three times/week for up to 16 weeks) is also a reasonable choice.
- •
Recalcitrant cases may be treated with ablative lasers.
- •
Destructive modalities (e.g., LN 2 , electrodessication) may be utilized but can cause scarring, and for this reason, such modalities are often avoided on the face.
Clinical Course
Most verrucae plana will resolve without treatment, usually over 2 to 3 years. EV often persists longer and also has the potential to eventuate into squamous cell carcinoma, on occasion.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


