Fig. 39.1
(a) Extreme herniation of the mammary gland into an expanded areolar sack. The inframammary fold (IMF) is very cranialized, with an absent inferior pole. (b) Circular constriction of the small base of the mammary gland, the cutaneous-glandular detachment, and the cutaneous laxity with the absence of Cooper’s ligaments. Due to the gravity of this case, one can intuitively exclude the possibility to correct the defect with the use of lipofilling only; therefore the use of mammary implant, in this case, is a necessity
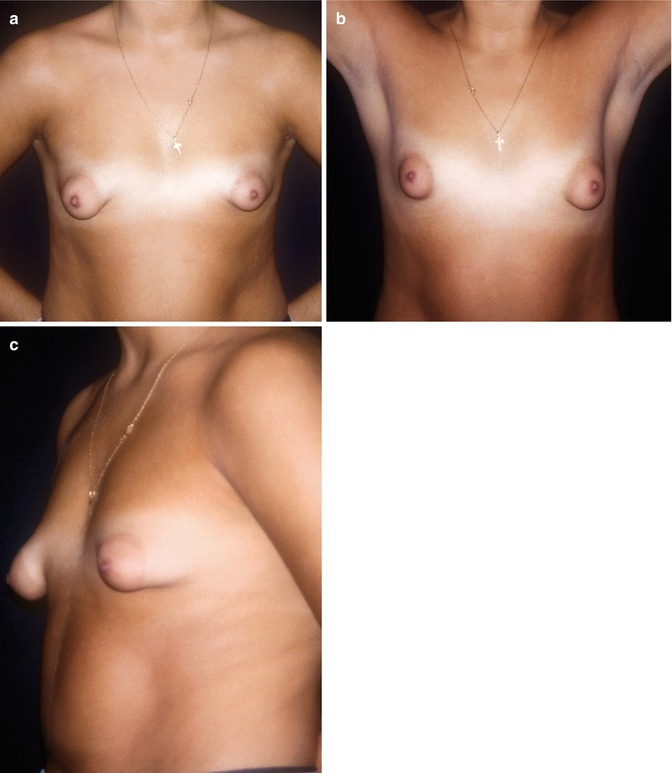
Fig. 39.2
(a–c) Bilateral tuberous breast type I, with a slight asymmetry, which shows all the anatomical characteristics typical of this malformation
1.
Glandular tissue “herniating” into an expanded areola
2.
Lack of cutaneous-glandular adhesions with Cooper’s ligament laxed or almost absent
3.
Certain degree of cutaneous laxity sometimes extremely relaxed
4.
Absence of the inferior pole
5.
Cranialized and tense inframammary fold with short distance between the nipple and the inframammary fold
Tuberous breast type II (Fig. 39.3): The main anatomical characteristics corresponding to this type of deformity are:
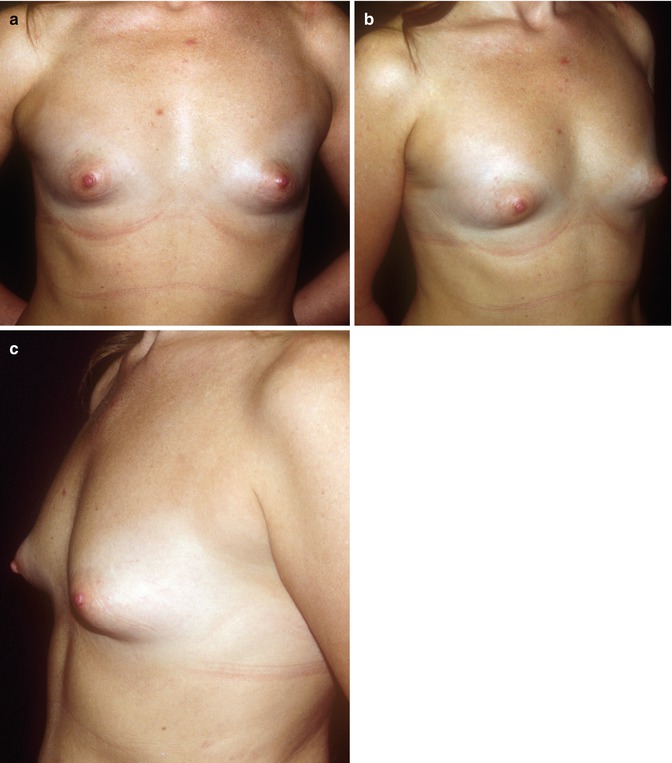
Fig. 39.3
(a–c) Hypoplastic tuberous breast. The right breast presents the most significant characteristic of tuberous breast type II that is a small areola, tense skin and subcutaneous tissue, concave inferior pole, and absence of IMF
1.
Glandular tissue protruding retro-areolarly, small or very small areola
2.
Firm skin with strong cutaneous-glandular adherence with fibrotic Cooper’s ligaments
3.
Inferior pole completely flat or concave
4.
Nipple-areolar complex (NAC) extremely lateralized on the thorax
This can be considered the ideal situation to be corrected with lipofilling only.
Tuberous breast type III: The main anatomical characteristics corresponding to this type of deformity are:
1.
Breast generally more or less normoplastic
2.
Morphological appearance of “tubular type,” with a dive-like ptosis
3.
With a NAC downward caudally positioned
4.
Reduced nipple-inframammary distance
5.
Mammary footprint fairly high on the thorax
Very frequently this type of tuberous breast deformity is present in asymmetric cases associated with tuberous breast type II on the contralateral side. It is curious to note that nearly always, in asymmetric cases, the authors find tuberous breast type II on the right side and tuberous breast type III on the left side.
Figure 39.4 shows a patient with tuberous breast type III. This patient could be treated completely and exclusively with lipofilling only, granted that the patient does not ask for an excessive increment in volume. This patient presents eating disorder and depression that could increase the risk of “failure” of the result due to her scarce skin quality, typical of patients presenting with these types of problems. Tuberous breast type II is on the right side and tuberous breast type III on the left side.
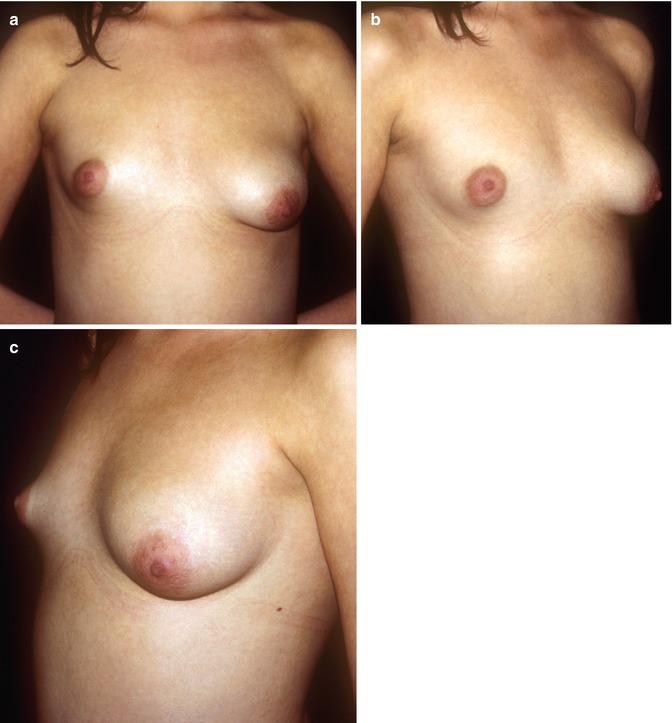
Fig. 39.4
(a–c) Asymmetric tubular breast with type II on the right side and type III on the left side. This can be completely corrected with lipofilling only
Figure 39.5
 Stem Cell Applications: An Overview
Stem Cell Applications: An Overview
 The Adipose Organ: Morphological Perspectives of Adipose Tissues
The Adipose Organ: Morphological Perspectives of Adipose Tissues
 The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
 Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
 Hand Rejuvenation with Stem Cell Fat Transfer
Hand Rejuvenation with Stem Cell Fat Transfer
 Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell




Related posts:
Stem Cell Applications: An Overview
The Adipose Organ: Morphological Perspectives of Adipose Tissues
The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
Hand Rejuvenation with Stem Cell Fat Transfer
Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
