A careful history
Physical findings (e.g., linear excoriations and crusts) (Fig. 11-1)
Appropriate symptom directed lab tests
 Figure 11-1 Pruritus, chronic. The upper back is a common place to find excoriations, crusts, and areas of linear pigmentary alterations that are indicative of chronic itching and scratching. |
Relies on establishing the cause and then either treating or removing it
Specific therapy for any underlying skin or internal disease
Ice packs to cool the skin
Menthol/camphor lotions
Regular use of emollients, especially if skin is dry
Topical corticosteroids for short periods
Topical calcineurin inhibitors such as tacrolimus 0.1% ointment (Protopic) or pimecrolimus 1% cream (Elidel) for itch associated with inflammatory skin conditions
Topical dapsone 5% cream (Zonalon)
Crisaborole 2% ointment (Eucrisa)
Topical hypochlorous acid-based topical prescription products (Levicyn™ Antipruitic Gel, or Dermal Spray)
Antihistamines—most useful in urticaria in which histamine is released but are not very effective for pruritus. However, sedating antihistamines can be used primarily for their sedative effects
Doxepin and amitriptyline—tricyclic antidepressants that have antipruritic action
Antiepileptic drugs—sodium valproate, gabapentin, and pregabalin
Dupixent, a monoclonal antibody that binds to the alpha subunit of the interleukin-4 receptor (IL-4Rα) and modulates both IL-4 and IL-13 signaling, appears to be highly effective for pruritus, though it is not yet officially approved for this indication
Broadband ultraviolet B or narrow-band UVB phototherapy alone, or in conjunction with UVA, has been shown to be helpful for pruritus associated with chronic kidney disease, psoriasis, atopic eczema, and cutaneous T-cell lymphoma
Scabies should be considered if more than one family member itches
Hodgkin disease may present with pruritus of unknown origin that precedes the diagnosis by up to 5 years
Topical antihistamines should not be used for chronic itch because they may sensitize the skin and result in allergic contact dermatitis
Intermittent itching in a specific place; typically, on the lower or mid-scapula
The localization and postinflammatory hyperpigmentation that sometimes results from the chronic rubbing and scratching reveals the diagnosis and is often the only clinical finding (Fig. 11-2)
Topical corticosteroids, topical anesthetics (e.g., pramoxine or lidocaine), and oral gabapentin as well as acupuncture bring variable results
Capsaicin cream (Zostrix), which depletes nerve endings of their chemical transmitters, applied three to five times daily may decrease symptoms
There have been case reports of successful treatment with botulinum toxin type A for this condition; however, treatment is often futile
 Figure 11-2 Notalgia paresthetica. Note the typical location on the lower scapula. The postinflammatory hyperpigmentation resulted from the chronic rubbing and scratching of this itchy spot. |
Nodules, cystic lesions, pustules (Fig. 11-3)
Healing with hypertrophic as well as atrophic scars
Abscesses and interconnecting sinuses may result
See Cheeks
Treatment may require a combination of medications that includes oral antibiotics, intralesional steroid injections, and possibly hormonal therapy in women
If all else fails, the recommended treatment for nodulocystic acne is oral isotretinoin (formerly known as Accutane), which, if started early, may prevent scarring. The treatment is required for at least 5 months, and repeated courses are sometimes necessary
 Figure 11-3 Nodulocystic acne. Erythematous papules, nodules, and scars. |
Elevated, firm, shiny, hairless, papules, or nodules; may be flesh-colored or tan
Lesions that are inflamed are usually of recent onset. They may be red or purple in color (Fig. 11-4)
Most often, they arise on the sternum (Fig. 11-5), the deltoid region of the upper arm, shoulders, and upper back
The most common sites on the head and neck are the earlobes, nasal alae, mandibular border, and posterior neck
Unlike keloids, the hypertrophic scar reaches a certain size and subsequently stabilizes or regresse, whereas keloids do not regress without treatment and tend to recur after excision
 Figure 11-4 Hypertrophic acne scars. These inflammatory scars are secondary to healed acne lesions. |
 Figure 11-5 Hypertrophic acne scars. Inflammatory acne scars on the sternum. |
Clinical appearance
Advise patient to discontinue or avoid repetitive skin trauma such as tattooing and skin-piercing practices, particularly in areas that are prone to abnormal scarring such as the presternal areas and earlobes
Topical corticosteroids: clear surgical tape impregnated with flurandrenolide (Cordran Tape) has been shown to soften and flatten hypertrophic scars over time
Intralesional corticosteroid injections (triamcinolone 10 to 40 mg/mL); these injections are also useful for diminishing pruritus and tenderness
Pulsed-dye lasers and resurfacing lasers such as CO2 laser and Erb:Yag and nonablative fractional lasers have been used successfully on some persistent hypertrophic scars
Uncontrolled overgrowth of scar tissue with extension beyond the site of the original wound with a tendency to send out “claw-like” prolongations (Fig. 11-6)
Usually asymptomatic, although some are pruritic and others may be quite painful and tender
Keloids, by virtue of their excessive size, are generally of great cosmetic concern to patients
Clinical appearance
Intralesional corticosteroid injections with triamcinolone acetate, often in concentrations as high as 40 mg/mL per treatment, can help flatten keloids and diminish itching and erythema. A 27- to 30-gauge needle at 4- to 6-week intervals often helps to flatten the lesions (Fig. 11-7). Overtreatment may result in skin atrophy, telangiectasias, and overdepressed scars (Fig. 11-8)
Excision using aseptic operative technique in combination with other postoperative modalities, such as triamcinolone acetate injections, compression dressings, silicone sheeting, radiotherapy, topical imiquimod cream, or injected interferon
Lasers have been used as alternatives to excision. As with excisional therapy, laser results are best when combined with postoperative injected steroids
There is recent evidence that dupilumab (Dupixent), which is an effective treatment for atopic dermatitis, may be beneficial in managing keloids
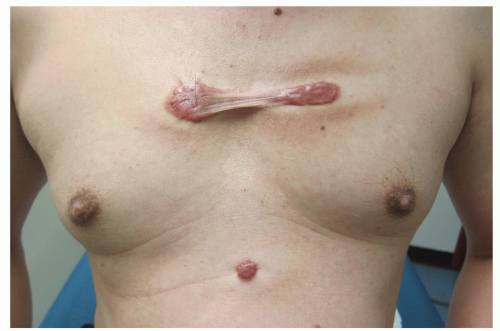 Figure 11-6 Keloid. Presternal keloid. |
 Figure 11-7 Keloid. Keloids being injected into this patient’s presternal lesions with intralesional triamcinolone. |
 Figure 11-8 Keloid. Keloid after intralesional cortisone injection. This shiny scar shows the possible untoward aftereffects of intralesional steroid injections—atrophy and telangiectasias. |
Table 11-1 Commonly Implicated Drugs for Different Drug Reactions | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Reactions often occur suddenly with or without fever and are often indistinguishable from viral exanthems
Lesions are pink, red, or purple in color (Fig. 11-9)
May become confluent in a symmetric, generalized distribution that often spares the face
Itching is common. The mucous membranes, palms, and soles may be involved
The onset occurs 7 to 10 days after starting the responsible drug, but sometimes may not appear until after the drug is discontinued
An eruption may last for 1 to 2 weeks and then fade
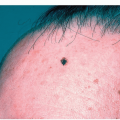
Lesions generally appear on the trunk as monomorphic acne-like papules and pustules (Fig. 11-10)
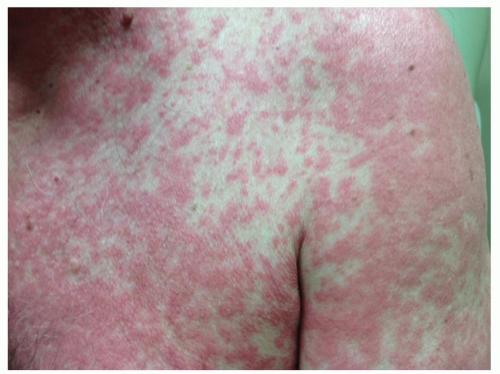 Figure 11-9 Morbilliform drug reaction. Note the “drug red” color of this confluent eruption caused by a penicillin derivative. |
 Figure 11-10 Acneiform drug reaction. Acneiform eruption caused by oral corticosteroids. This patient developed multiple monomorphic acne-like papules in a characteristic distribution. |
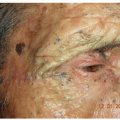
 Figure 11-11 Phototoxic drug reaction. Erythematous phototoxic (exaggerated sunburn) reaction in a person who was taking a tetracycline derivative and fell asleep on the beach. |
Lesions appear in sun-exposed areas such as the “V” of the neck, upper sternum, extensor forearms, and the face as an exaggerated sunburn (Fig. 11-11)
Obtaining a detailed, careful history is paramount
A drug-induced reaction should be considered in the differential diagnosis of any symmetric cutaneous eruption with sudden onset in a patient who takes medications
Skin biopsy of an exanthem showing perivascular lymphocytes and eosinophils may be helpful, but not diagnostic
Patch tests are useful in diagnosing allergic contact dermatitis (see Appendix: Diagnostic and Therapeutic Techniques)
Often, the decision whether to continue or discontinue a potentially vital drug presents a dilemma
The presence of urticaria, mucosal involvement, extensive or palpable purpura, or blisters almost always requires discontinuation of the responsible drug
Oral antihistamines such as diphenhydramine (Benadryl), hydroxyzine (Atarax), or the nonsedating agents such as cetirizine (Zyrtec) or loratadine (Claritin) may be helpful
Systemic steroids are given only in severe cases in which an infectious etiology is ruled out
A drug eruption may easily be confused as being a feature of the condition that it is intended to treat (e.g., a viral exanthem treated with an antibiotic)
If it is necessary to continue a responsible drug (i.e., there is no alternative medication) and the adverse reaction is mild or tolerable, the difficulty can be minimized by decreasing the dosage or treating the adverse drug reaction
If a patient is taking multiple medications, it is sometimes difficult to identify the specific agent that is responsible for an adverse reaction. In these instances, a reference guide to drug eruptions and interactions could suggest the most likely suspect drug
An ADR can occur days after a drug has been discontinued
ADRs from systemic medications tend to be symmetrical in distribution; however, certain eruptions have specific regional predilections (e.g., fixed drug eruptions and erythema nodosum)
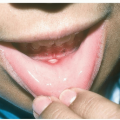
Wheals are the color of the patient’s skin or appear pale red
Pruritus without excoriations
Annular or gyrate shapes (Fig. 11-12)
Individual lesions, by definition, last less than 24 hours (evanescent wheals)
Overall, acute urticarial episodes can last for days (generally less than 30 days)
Lesions may be accompanied by a deeper swelling (angioedema)
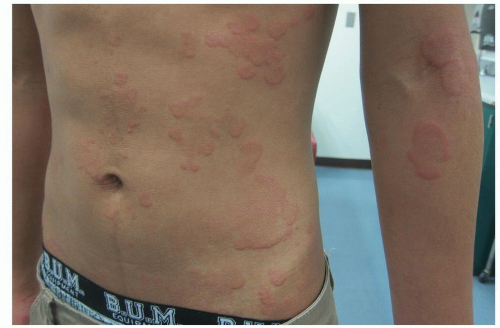 Figure 11-12 Urticaria. Lesions are annular, arciform, and polycyclic, with bizarre shapes. |
The diagnosis is usually made on clinical observation and history
If possible, the cause of the hives should be determined and eliminated
Treatment is symptomatic with antihistamines, cool soaks, and ice packs
Over-the-counter first-generation sedating antihistamines, such as histamine H1 blockers: hydroxyzine (Atarax), diphenhydramine (Benadryl), and cyproheptadine (Periactin)
Over-the-counter second- and third-generation less-sedating antihistamines: loratadine (Claritin), fexofenadine (Allegra), cetirizine (Zyrtec), and levocetirizine (Xyzal), may be used during the daytime
Antihistamines can be used at up to four times the standard dose in the treatment of urticaria
A more sedating H1/H2 blocker such as doxepin (Sinequan) can be prescribed at a much lower dosage than when it is used as an antidepressant, especially at bedtime
 Alert: Anaphylaxis or an anaphylactoid reaction can occur
Alert: Anaphylaxis or an anaphylactoid reaction can occur Alert: Epinephrine, which is sometimes administered by intramuscular or subcutaneous injection for acute urticaria, should not be used for routine cases of hives; rather, it should be reserved for cases of acute anaphylaxis
Alert: Epinephrine, which is sometimes administered by intramuscular or subcutaneous injection for acute urticaria, should not be used for routine cases of hives; rather, it should be reserved for cases of acute anaphylaxis Alert: Patients who have severe anaphylactic reactions should consider wearing a Medic Alert Bracelet that describes their problem
Alert: Patients who have severe anaphylactic reactions should consider wearing a Medic Alert Bracelet that describes their problem
The morphology and duration—less than 24 hours—of individual lesions is similar to that of acute urticaria; however, the condition, by definition, lasts for more than 6 weeks
Patients may also experience a coexistent physical urticaria such as dermatographism (see below)
Symptoms may continue for weeks, months, or years; however, in most cases the disease ends spontaneously
The diagnosis is usually made on clinical observation and history
A symptom-directed search for an underlying illness (e.g., systemic lupus erythematosus, thyroid disease, and lymphoma) should be undertaken
If a complete review of systems is normal and a physical urticaria is ruled out, some the following laboratory tests may be obtained to determine a cause: CBC, ESR, ANA, thyroid function studies, stool examination for ova and parasites, hepatitis-associated antigen test, assessment of the complement system, and RAST test for immunoglobulin E antibodies
Antihistamines (see under Acute Urticaria above)
Systemic steroids are sometimes helpful for temporary relief but should be used with caution
Food testing and elimination diets are rarely helpful
Montelukast (Singulair), a leukotriene receptor antagonist, has also been used for urticaria
Cyclosporine and mycophenolate mofetil (CellCept) have demonstrated temporary improvement
The biologic omalizumab (Xolair) has also shown positive results with chronic idiopathic urticaria; however, urticaria has tended to recur. It should be administered with caution in regard to rare cases of anaphylaxis
Aspirin/NSAIDs, opiates, and stress tend to exacerbate CIU
Determining an underlying cause for CIU is often a futile search
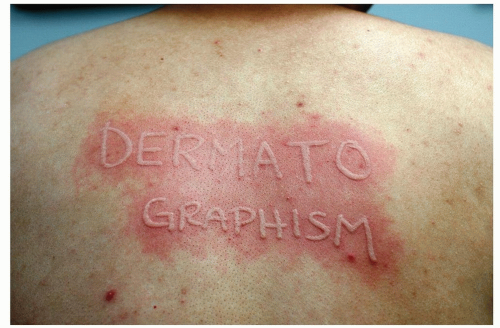 Figure 11-13 Dermatographism (“skin writing”). These lesions occurred 3 minutes after stroking with the wooden tip of a cotton swab. |
Dermatographism (“skin writing”): urticaria that results from firm stroking or from scratching the skin. It can also be elicited by wearing tight garments (e.g., bras) (Fig. 11-13)
Cold urticaria: itchy hives occur at sites of cold exposure caused by cold winds or immersion in cold water
Solar urticaria: from sun exposure (Fig. 11-14, A and B)
Cholinergic urticaria: brought about by heat or exercise
Lesions often annular with peripheral enlargement and central clearing (Fig. 11-15)
Begins as a pruritic, circular or oval, erythematous, scaling patch or plaque that spreads centrifugally
Central clearing follows, while an active, advancing, raised border remains. The result is an annular (ring-shaped) plaque from which the disease derives its common name (“ringworm”)
Single or multiple lesions
May be pruritic or asymptomatic
 Figure 11-14 Solar urticaria A and B. Solar urticaria induced by ultraviolet A light. A, Before sun exposure. B, After 15 minutes of sun exposure through a window. |
 Figure 11-15 Tinea Corporis. Annular plaques with peripheral scale on border. |
A history of a newly adopted kitten, or of another infected contact, is helpful
Diagnosis is confirmed by a positive potassium hydroxide (KOH) examination or fungal culture best taken from the “active border” of a lesion or from periodic acid-Schiff stain on biopsy specimens
A fungal culture is an alternative, albeit slower, method for diagnosis
Topical antifungal agents such as ketoconazole 2% cream twice daily
Systemic antifungal agents such as terbinafine (Lamisil), itraconazole (Sporanox), ketoconazole, or griseofulvin are sometimes necessary
If pets appear to be the source of infection, they may also need antifungal treatment after evaluation by a veterinarian
Initially, the LB lesion is a red macule or papule at the site of a tick bite. The bite itself usually goes unnoticed. Approximately 2 to 30 days after infection, the rash appears
Common sites are the trunk, groin, and thigh
Usually asymptomatic, the initial lesion expands to form an annular erythematous lesion, erythema migrans, which is the classic lesion of LB (Fig. 11-16)
Typically measures from 4 to 70 cm in diameter, generally with central clearing
The center of the lesion, which corresponds to the putative site of the tick bite, may become darker, vesicular, hemorrhagic, or necrotic

Figure 11-16 Acute Lyme Disease, erythema migrans.
A solitary, annular, target-like, erythematous plaque of erythema migrans.

Figure 11-17 Acute Lyme Disease, erythema migrans.
Multiple annular lesions of erythema migrans are seen here.
Lesions may be confluent (not annular), and concentric rings may form
Multiple lesions sometimes occur, likely the result of bacteremia (Fig. 11-17)
At the early stage of disease, flu-like symptoms, such as malaise, arthralgias, headaches, and a low-grade fever and chills, may develop
Some of the signs and symptoms of LB may not appear for weeks, months, or even years after the initial tick bite and are believed to be caused by immunopathogenic mechanisms. They include arthritis, nervous system problems, Bell palsy, headaches, memory loss, and cardiac dysrhythmias
Rarely, a lesion of lymphocytoma cutis or acrodermatitis chronica atrophicans appears
Late Lyme disease refers to symptoms, primarily rheumatologic and neurologic, that occur months to years after initial infection
A history of tick exposure or bite in an endemic area
Most patients at the erythema migrans stage are seronegative
Currently, CDC recommends a two-step testing procedure. The first step typically consists of a screening enzyme immunoassay (EIA) or enzyme-linked immunosorbent assay (ELISA); if results are positive or equivocal, a Western immunoblot test is performed to confirm the results. Testing should be repeated after about 1 month if negative, because the test may be negative shortly after exposure
Ixodes ticks are much smaller than dog ticks. In their larval and nymphal stages, they are no bigger than a pinhead
Unengorged adult ticks are the size of the head of a match (Fig. 11-18)
An attached tick should be removed carefully by using a pair of tweezers. The tick should be grasped by the head (not the body) as close as possible to the skin, to avoid force that may crush it
Doxycycline (100 mg twice per day for 21 days [do not use in children younger than 10 years or in pregnant women]) or
Amoxicillin (500 mg three times per day for 21 days) or
Ceftriaxone (Ceftin) or cefuroxime (500 mg twice per day for 21 days [expensive; use if patient is unable to tolerate the other antibiotics])
Azithromycin (Zithromax) and erythromycin: second-line drugs that should be considered for those who are allergic to beta-lactam antibiotics
People who are outdoors in endemic areas in the summer should wear long pants and socks, use insect repellents, and frequently examine themselves and their clothing for ticks
Doxycycline: a single dose of 200 mg given in less than 72 hours of tick removal is reported to prevent the disease
In endemic areas, patients with probable erythema migrans and a recent source of tick exposure should be started on treatment without blood tests.
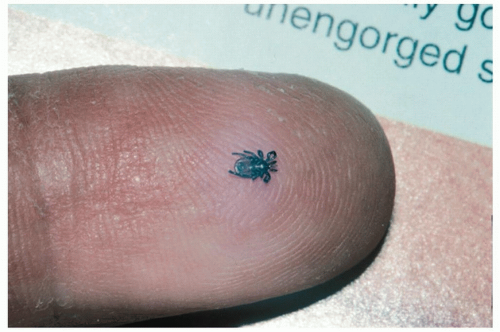 Figure 11-18 Acute Lyme Disease, Ixodes tick. An adult tick is the size of the head of a match.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|