3 Treatment of Squamous and Basal Cell Carcinoma of the Skin Basal cell and squamous cell skin cancers, collectively known as nonmelanoma skin cancers (NMSCs), are the most common cancer in the United States. An estimated 5 million cases of NMSC are diagnosed annually; this exceeds the incidence of all other cancers combined.1,2 In the United States alone, the diagnosis and treatment of NMSCs has increased dramatically with a growth rate of 77% over the past two decades. The average annual number of adults treated for skin cancer increased from 3.4 million in 2002–2006 to 4.9 million in 2007–2011. During this period, the average annual total cost for skin cancer increased from $3.6 billion to $8.1 billion, representing an increase of 126.2%, while the average annual total cost for all other cancers increased by 25.1%. During 2007–2011, nearly 5 million adults were treated for skin cancer annually, with average treatment costs of $8.1 billion each year, about $4.8 billion for NMSCs and $3.3 billion for melanoma.2,3 While surveillance and diagnosis has continued to improve, the incidence of this common malignancy also appears to be rising rapidly.4 Basal cell carcinomas (BCCs) are roughly four to five times more common than squamous cell carcinomas (SCCs). More than 2.8 million new cases of BCC are diagnosed each year in the United States alone, and are estimated to result in more than 3,000 deaths.5,6,7 Although rarely metastatic, BCC and SCC can produce substantial local invasion and destruction along with disfigurement and may involve extensive areas of underlying soft tissue, cartilage, and bone. Cutaneous squamous cell carcinoma (cSCC) is the second most common NMSC worldwide. While most of these lesions can be successfully managed with excision, there is a subset of lesions that metastasize, leading to severe morbidity and mortality. While small, the number of cSCCs that metastasize has been compared to the metastatic rate of renal and oropharyngeal carcinomas.8 The skin is a complex organ made up of multiple cell types and many of these cell types can undergo malignant transformation at various points in their differentiation, leading to tumors with distinct histology and dramatically different biological behaviors, such as SCC and BCC. The outer layer or epidermis is made primarily of keratinocytes but has several other minor cell populations. The bottom layer is formed of basal keratinocytes abutting the basement membrane. The basement membrane is formed from products of keratinocytes and dermal fibroblasts, such as collagen and laminin, and is an important anatomical and functional structure. As the basal keratinocytes divide and differentiate, they lose contact with the basement membrane and form the spinous cell layer, the granular cell layer, and the keratinized outer layer or stratum corneum. The true cytologic origin of BCC remains in question; however, BCC and basal cell keratinocytes share many histologic similarities. Alternatively, the outer root sheath cells of the hair follicle have also been proposed as the cell of origin for BCC.9,10 This is suggested by the fact that BCCs occur predominantly on hair-bearing skin. BCCs rarely metastasize but can invade tissue locally or regionally, with a potential for perineural invasion and rapid spread. A tendency for superficial necrosis in the center in the lesion has resulted in the characteristic name “rodent ulcer,” frequently used to describe such growths. Similarly, debate remains about the origin of SCC; however, the leading hypothesis illustrates the derivation of cutaneous SCC from epidermal stem cells associated with the hair follicles.11 A variety of tissues, such as lung and uterine cervix, also give rise to SCC, with varying characteristics depending on the tissue source. SCC derived from different anatomic locations can have moderately differing aggressiveness and expected clinical course; for example, SCC from glabrous (smooth, hairless) skin frequently has a lower metastatic rate than SCC arising from the vermillion border of the lip or from scars.12 Estimates of the incidence of BCC are imprecise, given there is currently no central registry that collects data on BCC occurrence. Lower estimates cited by The American Cancer Society estimates that more than 2 million NMSCs were treated in the United States in 2006. However, a population-based study estimated a higher number of lesions, reporting that approximately 3.5 million NMSCs were treated in the United States during the same year.1 Additionally, several incidence-based mathematical models support a higher prevalence of NMSC in the United States.13 According to the model, approximately 13 million white non-Hispanic individuals living in the United States in 2007 may have had a personal history of at least one NMSC. Individuals with a history of BCC are at increased risk for subsequent lesions. Approximately 40% of patients who have had one BCC will develop another lesion within 5 years.14,15 Multiple epidemiologic observations provide insights into the etiology of BCC. Namely, BCC is particularly common in Caucasians and very uncommon in blacks and other dark-skinned populations. In white populations in the United States, the incidence of BCC has increased by more than 10% per year, and the lifetime risk of developing a BCC is estimated at 30%.16,17,18 An increasing incidence has also been noted in other countries, such as Canada, Finland, and Australia,19,20,21 with evidence of increasing incidence of aggressive-growth histologic subtypes.22 There is notable geographic variation in incidence, likely secondary to environmental exposures and protection strategies. States closer to the equator, such as Hawaii and California, have an incidence of BCC at least twice that of the Midwestern United States.23,24,25 There are also prominent global variations in incidence. Northern European countries, such as Finland, have an incidence one-fourth that of the Midwestern United States versus Australia where rates are 40 times that of Finland.19,26 Men have a 30% higher incidence than women and also a higher incidence of superficial type BCC.19,23,27,28 The incidence of BCC increases with age; persons aged 55 to 75 have about a 100-fold higher incidence of BCC than those younger than 20.29 Although an aging population with higher life expectancies may account for part of the increasing incidence of BCC, the incidence of BCC among Americans younger than 40 also appears to be increasing, particularly among women.4 In the United States, the average age of onset of cutaneous SCC is 65 years;30 however, there are increasing reports of patients as young as 20 to 30 years of age in regions of higher ultraviolet (UV) exposure such as Florida and southern California. There is a predilection for males, but the incidence of SCC originating on the legs is greater in females. Factors that increase the risk for SCC include Fitzpatrick skin types I and II, outdoor occupations such as farming and construction work, and exposure to human papillomavirus (HPV) types 16, 18, and 31.31 Exposure to UV radiation and sunlight is the greatest risk factor, as illustrated in studies showing a direct correlation between psoralen plus ultraviolet A light (PUVA) exposure and the incidence of SCC.32,33,34,35 In this study, the relative risk for developing SCC in patients with 350 to 450 PUVA treatments compared with less than 50 treatments was 6.01.13,34 Treatment with PUVA increases the risk for SCC by two mechanisms, which refer to, respectively, its mutagenic effects and its immunosuppressive effects. Overall, SCC is uncommon in dark-skinned individuals, but it remains the most common cutaneous cancer in African-Americans. In such individuals, the cancer usually occurs in areas that are not sun exposed.36 Darkly pigmented skin possesses greater amounts of melanin in the epidermis, which partially protects against the carcinogenic effects of UV light. As a result, sun exposure is a less common etiology. As in the overall population, SCC in darker skin is often preceded by the development of actinic keratosis (AK).37,38 BCC is a common skin cancer arising from the basal layer of epidermis and its appendages. These tumors have been referred to as “epitheliomas” because of their low metastatic potential. However, the term carcinoma is appropriate, since they are locally invasive, aggressive, and destructive of skin and the surrounding structures including bone. Sun exposure is the most important environmental cause of BCC, and most risk factors relate directly to a person’s sun exposure habits or susceptibility to solar radiation. These risk factors include having fair skin, light-colored eyes, red hair, northern European ancestry, older age, childhood freckling, and an increased number of past sunburns.39,40,41 The type, quantity, and timing of sun exposure associated with an increased risk of BCC are not clearly defined. Childhood sun exposure appears to be more important than exposure during adult life.40,42 In a Canadian case control study that included 226 men with BCC and 406 age-matched controls, the development of BCC was strongly correlated with childhood and adolescent sun exposure but not cumulative or recent sun exposure.42 In other studies, however, adult sun exposure also was a risk factor for BCC.41 It has been estimated that aggressive sun protection before the age of 18 years could reduce the number of NMSCs by almost 80%.43 Several trials provide evidence that sunscreen use decreases the incidence of SCCs and that there are no adverse effects from sunscreen use.44,45 However, a randomized trial evaluating the effects of sunscreen and the antioxidant beta carotene over a 4-year period found that those using topical sunscreen had a 40% reduction in SCCs but no decrease in BCCs.46 The frequency and intensity of sun exposure may also be important. Solar exposure in intermittent, intense increments increases the risk of BCC more than a similar dose delivered more continuously over the same period of time.47 Evidence in renal transplant recipients provides additional support to the concept that acute or intermittent sun exposure increases the risk of BCC.48 Additionally, indirect support for an important role for sun exposure is derived from a large, nested case–control study of female nurses.49 In the study, a contributory role of extensive sun exposure was suggested by the finding that women in the highest quartile for baseline serum vitamin D levels were at greater risk for the subsequent development of BCC than women in the lowest quartile (odds ratio [OR] 2.07; 95% confidence interval [CI]: 1.52–2.80). The authors proposed that the plasma vitamin D level was a potential indicator of the degree of long-term sun exposure. The use of tanning beds may increase the risk for early development of BCC.50,51,52,53,54 A cohort study of approximately 73,000 female nurses found that women who used tanning beds more than six times per year during high school or college were more likely to develop BCC than women who did not use tanning booths during these time periods (adjusted hazard ratio 1.73; 95% CI: 1.52–1.98).55 A contribution of UV light exposure from indoor tanning to BCC is also suggested by the results of a 2012 meta-analysis of observational studies.53 Subjects with a history of any tanning bed use were more likely to develop BCC than those who had never used tanning beds (relative risk 1.29; 95% CI: 1.08–1.53). The relative risk for BCC for individuals who began tanning prior to age 25 was 1.40 (95% CI: 1.29–1.52). A subsequent population-based case–control study, including approximately 650 cases of BCC and 450 controls, found that tanning bed users had a 60% increased risk of developing a BCC at or before the age of 50 years (OR 1.6; 95% CI: 1.3–2.1).54 The risk was doubled for those reporting a first use of tanning devices before the age of 20. Superficial multicentric BCC occurs 30 to 40 years after chronic exposure of arsenic, which may occur as a result of ingesting contaminated drinking water, seafood, or medications.56,57,58,59 Superficial therapeutic ionizing radiation, as for facial acne, psoriasis, or tinea capitis, increases the risk of NMSC, including BCC.60,61 The latency period for development of BCCs is estimated to be approximately 20 years, and lesions are limited to sites with radiation exposure. Due to the advent of other effective therapies, the use of ionizing radiation for the treatment of inflammatory skin conditions has declined. Ionizing radiation used to treat childhood cancers also increases the risk for the subsequent development of BCC. This was illustrated in a study of 776 subjects documenting an approximately 10-fold higher rate of BCC than was expected in this population.62 All of the BCCs were located within the radiation field. In addition, a case–control study of 199 patients with a history of both childhood cancer and BCC and 597 controls with a history of childhood cancer without BCC found a linear dose–response relationship between the radiation dose and risk for BCC. An increase in risk was detected among patients who received at least 1 Gy of radiation to the skin, and patients who received 35 Gy or more were 40 times more likely to develop BCC than those who were not treated with radiation (OR 39.8; 95% CI: 8.6–185). The treatment of other noncutaneous disorders with radiation therapy (RT) has also been associated with the appearance of BCC.60,63,64 Studies of survivors of the atomic bomb explosions in Japan support the role of exposure to ionizing radiation in the development of BCC. In a retrospective study of bomb survivors, the incidence of subsequent BCC increased with proximity to the hypocenter of the explosion.65 Therapeutic exposure to PUVA for cutaneous disorders such as psoriasis increases the risk of NMSC, particularly SCC.66,67 The risk of BCC in patients treated with PUVA is lower than the risk for cutaneous SCC. In a 30-year prospective cohort study documenting the incidence of NMSC in patients given PUVA for psoriasis, the increase in risk for BCC was modest compared with cutaneous SCC.68 The association of BCC with UV light exposure has led to questions about the impact of photosensitizing drugs on development of BCC. An association between prior use of photosensitizing tetracyclines or diuretics and increased risk for BCC has been documented in several observational studies.69,70 In addition, an American population-based case–control study of 1,567 adults with BCC and 1,906 controls found a minor increase in risk for multiple BCC (OR 1.4; 95% CI: 1–2.1) and BCC before the age of 51 (OR 1.5; 95% CI: 1.1–2.1) among participants who recalled use of a photosensitizing medication.69 Additional studies are necessary to clarify the relationship between photosensitizing drugs and BCC. Chronic immunosuppression (as occurs with solid organ transplantation and with human immunodeficiency virus [HIV] infection) may increase risk for the development of BCC, although the increase in risk is less than that observed for SCC.71 The risk for BCC after solid organ transplantation appears to increase linearly over time, whereas the risk for SCC rises exponentially.72,73 The increased risk for skin cancer in organ transplant recipients is attributed to chronic exposure to immunosuppressive agents. The specific impact of systemic glucocorticoid therapy on BCC risk is uncertain; studies performed in patients without a history of organ transplantation conflict on whether systemic glucocorticoid therapy significantly increases risk for BCC.73,74,75 Support for an increased risk for BCC among HIV-positive individuals was demonstrated in a retrospective cohort study of HIV-positive (n = 6,560) and HIV-negative (n = 36,821) non-Hispanic white patients. The study found that patients with HIV infection were approximately twice as likely to develop BCC than patients without HIV infection (adjusted rate ratio 2.1; 95% CI: 1.8–2.3).76,77 A personal history of BCC or SCC is strongly associated with subsequent BCC or SCC.15 There is an approximate 20% increased risk of a subsequent lesion within the first year after a skin cancer has been diagnosed.15,78,79 The mean age of occurrence for these NMSCs is the mid-60 s.14,15 In addition, several studies have found that individuals with a history of skin cancer have an increased risk of a subsequent diagnosis of a noncutaneous cancer.80,81,82,83,84 In the absence of other risk factors or evidence of a defined cancer susceptibility syndrome, as discussed below, skin cancer patients are encouraged to follow screening recommendations for the general population for sites other than the skin. Genetic variation may play a role in susceptibility to BCC. Some gene sequence variants that are affiliated with increased risk of BCC also correlate with light skin pigmentation.85 In addition, genome-wide association studies have identified genetic variants (see below) that may influence BCC risk through other pathways, such as an effect on the growth or differentiation of basal layers of the epidermis or an effect on the P53 tumor suppressor gene or hedgehog pathways.86,87,88,89,90,91,92 Genes that affect the immune response may also impact susceptibility to BCC. Cytotoxic lymphocyte-associated antigen-4 (CTLA-4) is expressed on regulatory T cells and is involved in UV-induced immune tolerance. In a case–control study, genetic variation at the CTLA-4 locus influenced the risk of BCC, particularly among patients with a higher number of severe sunburns.93 The most significant genetic components for BCC are the PTCH1 and PTCH2 genes. PTCH1 mutations in the gene coding for the transmembrane receptor protein PTCH1, or PTCH, are associated with basal cell nevus syndrome (BCNS) and sporadic cutaneous BCCs. PTCH1, the human homolog of the Drosophila segment polarity gene patched (ptc), is an integral component of the hedgehog signaling pathway, which serves many developmental (appendage development, embryonic segmentation, neural tube differentiation) and regulatory (maintenance of stem cells) roles.94,95 In the resting state, the transmembrane receptor protein PTCH1 acts catalytically to suppress the seven-transmembrane protein Smoothened (SMO), preventing further downstream signal transduction.96,97 Stoichiometric binding of the hedgehog ligand to PTCH1 releases inhibition of SMO, with resultant activation of transcription factors (GLI1, GLI2), cell proliferation genes (cyclin D, cyclin E, myc), and regulators of angiogenesis.97,98 Thus, the balance of PTCH1 (inhibition) and SMO (activation) manages the essential regulatory downstream hedgehog signal transduction pathway. Loss-of-function mutations of PTCH1 or gain-of-function mutations of SMO tip this balance toward constitutive activation, a key event in potential neoplastic transformation. Demonstration of allelic loss on chromosome 9q22 in both sporadic and familial BCCs suggested the potential presence of an associated tumor suppressor gene.99,100 Further investigation identified a mutation in PTCH1 that localized to the area of allelic loss.101 Up to 30% of sporadic BCCs demonstrate PTCH1 mutations.102 In addition to BCC, medulloblastoma and rhabdomyosarcoma, along with other tumors, have been associated with PTCH1 mutations. All three malignancies are associated with BCNS, and most people with clinical features of BCNS demonstrate PTCH1 mutations, predominantly truncation in type.103 Truncating mutations in PTCH2, a homolog of PTCH1 mapping to chromosome 1p32.1–32.3, have been demonstrated in both BCC and medulloblastoma.104,105 PTCH2 displays 57% homology to PTCH1, differing in the conformation of the hydrophilic region between transmembrane portions 6 and 7, and the absence of C-terminal extension.106 While the exact role of PTCH2 remains unclear, there is evidence to support its involvement in the hedgehog signaling pathway.104 Nevus sebaceous ( Fig. 3.1 Nevus sebaceous (NS). In infancy and childhood, NS remains mostly unchanged, due to the quiescence of sebaceous glands. At puberty, under hormonal influences, lesions thicken and become verrucous or nodular. Rapid, circumscribed enlargement or ulceration should arouse suspicion for malignant transformation. Fig. 3.2 Nevus sebaceous (NS). The diagnosis of NS is usually based upon the clinical presentation. In most cases, NS is apparent at birth and presents as a well-defined, thin, yellow-orange or tan, oval, round, or linear plaque. Sometimes lesions are not noticed until later in childhood or after puberty. A biopsy for histopathologic confirmation may be warranted if the diagnosis is uncertain. The definitive treatment of NS is full-thickness excision. The decision to excise should be made in individual patients, based upon age, extension, and location of the lesion, and patient’s or parents’ concern about the cosmetic appearance and/or risk of malignancy. Fig. 3.3 Nevus sebaceous (NS). A variety of benign and malignant epithelial neoplasms may arise within NS. Benign tumors include trichoblastoma, syringocystadenoma papilliferum, trichilemmoma, sebaceoma, nodular hidradenoma, hidrocystoma, and eccrine poroma. Malignant neoplasms include basal cell carcinoma, apocrine carcinoma, trichilemmal carcinoma, sebaceous carcinoma, microcystic adnexal carcinoma, porocarcinoma, and squamous cell carcinoma. The exact incidence and the lifetime risk of malignancy arising in NS are unknown. The risk of malignancy increases with age, but basal cell carcinomas have been reported also in children. While most arise sporadically, BCC is also associated with several clinical syndromes including Bazex syndrome, Gorlin’s syndrome (BCNS), and highly UV-sensitive conditions such as xeroderma pigmentosum (XP). Constitutive activation of the sonic hedgehog signaling pathway is thought to play a significant role in the majority of BCC pathogenesis.110,111 Bazex syndrome is characterized by multiple BCCs and follicular atrophoderma.112 Rombo syndrome presents with atrophoderma vermiculatum and vellus hair cysts with milia-like appearance.113 Patients with XP are at increased risk for BCC as well as SSCs and melanomas. The incidence of these malignancies for individuals with XP under the age of 20 is approximately 2,000 times that seen in the general population.114,115,116 Individuals with BCCs and/or SCCs report a higher frequency of these cancers in their family members than do controls. The importance of this finding is unclear. Apart from defined genetic disorders with an increased risk of BCC, a positive family history of any skin cancer is a strong predictor of the development of BCC. Nevoid BCC syndrome is also known as the Gorlin–Goltz syndrome and is inherited in an autosomal dominant manner; however, approximately 30–50% of cases represent sporadic mutations.117,118,119 Its prevalence has been estimated at approximately 1 in 56,000 and manifests in young adulthood.120 In most cases, the abnormality is due to a mutation in the patched gene (PTCH) of chromosome 9 q22–q31, thereby resulting in upregulated proliferation.119,121,122 Currently, no genetic test has been developed for widespread use, and diagnosis remains based on clinical criteria. The diagnosis may be established with documentation of two major criteria or one major and two minor criteria123,124 ( The clinical features of nevoid BCC syndrome include the presence of numerous BCCs with a higher prevalence of nodular, superficial, and infundibulocystic types (
3.1 Introduction
3.2 Risk Factors for Basal Cell Carcinoma
3.2.1 Ultraviolet Radiation
3.2.2 Tanning Beds
3.2.3 Chronic Arsenic Exposure
3.2.4 Ionizing Radiation
3.2.5 Therapeutic Exposure
3.2.6 Photosensitizing Drugs
3.2.7 Immunosuppression
3.2.8 Previous Personal History of Nonmelanoma Skin Cancer
3.2.9 Nevus Sebaceous
![]() Fig. 3.1,
Fig. 3.1, ![]() Fig. 3.2,
Fig. 3.2, ![]() Fig. 3.3) is an uncommon congenital hamartoma of the skin composed of epidermal, follicular, sebaceous, and apocrine elements. BCC may develop within nevus sebaceous, though this occurrence is rare. BCCs are the most commonly reported malignant neoplasm occurring in roughly 0.5 to 7% of sebaceous nevi.107,108 In a retrospective study of 596 nevus sebaceous excisions from adults and children, BCC was detected in specimens from five adults (0.8%).109 A separate review of 631 children with 651 lesions of nevus sebaceous found that BCC may also develop within nevus sebaceous in children; BCC was found in excisional specimens from five patients (0.8%).107
Fig. 3.3) is an uncommon congenital hamartoma of the skin composed of epidermal, follicular, sebaceous, and apocrine elements. BCC may develop within nevus sebaceous, though this occurrence is rare. BCCs are the most commonly reported malignant neoplasm occurring in roughly 0.5 to 7% of sebaceous nevi.107,108 In a retrospective study of 596 nevus sebaceous excisions from adults and children, BCC was detected in specimens from five adults (0.8%).109 A separate review of 631 children with 651 lesions of nevus sebaceous found that BCC may also develop within nevus sebaceous in children; BCC was found in excisional specimens from five patients (0.8%).107



3.2.10 Inherited Disorders
3.2.11 Family History
3.2.12 Nevoid BCC Syndrome (Gorlin’s Syndrome)
![]() Table 3.1).
Table 3.1).
3.3 Clinical Features
![]() Fig. 3.4). Patients may also have cysts of the skin (steatocystomas) and bone, particularly the mandible (
Fig. 3.4). Patients may also have cysts of the skin (steatocystomas) and bone, particularly the mandible (![]() Fig. 3.5) and maxilla (odontogenic keratocysts).118,123 Also present are skeletal anomalies including spinal and rib deformities, excessive ossification of cranial bones and falx cerebri with concurrent frontal bossing and bridging of the sella turcica.118,123,125 Palmoplantar pits (
Fig. 3.5) and maxilla (odontogenic keratocysts).118,123 Also present are skeletal anomalies including spinal and rib deformities, excessive ossification of cranial bones and falx cerebri with concurrent frontal bossing and bridging of the sella turcica.118,123,125 Palmoplantar pits (![]() Fig. 3.6 and
Fig. 3.6 and ![]() Fig. 3.7) may appear during the second decade of life in addition to psychiatric or neurologic dysfunction including schizophrenia, mental retardation, and cerebellar degeneration.126,127 In the absence of distinct criteria, clinical suspicion of Gorlin’s syndrome may be indicated for any patient with multiple histologically proven BCCs arising at a young age. Morbidity and premature mortality in nevoid basal cell carcinoma syndrome (NBCCS) are primarily related to the development of skin cancers and other tumors associated with the syndrome.
Fig. 3.7) may appear during the second decade of life in addition to psychiatric or neurologic dysfunction including schizophrenia, mental retardation, and cerebellar degeneration.126,127 In the absence of distinct criteria, clinical suspicion of Gorlin’s syndrome may be indicated for any patient with multiple histologically proven BCCs arising at a young age. Morbidity and premature mortality in nevoid basal cell carcinoma syndrome (NBCCS) are primarily related to the development of skin cancers and other tumors associated with the syndrome.
Major criteria | Minor criteria |
Multiple (> 2) BCCs at any age or one BCC less than 20 y or > 10 BCCs | Congenital skeletal defects: bifid, fused, splayed, or missing rib, or bifid, wedged, or used vertebra |
Histologically proven odontogenic keratocyst or a polyostotic bone cyst | Cardiac or ovarian fibroma |
Palmar or plantar pits (3 or more) | Medulloblastoma |
Ectopic calcification: bilamellar or early (< 20 y) calcification of the falx cerebri | Large head with occipitofrontal circumference > 97th percentile, with frontal bossing |
Family history of basal cell nevus syndrome | Congenital malformation: cleft lip and/or palate, polydactyly, congenital eye defect such as cataract, microphthalmos or coloboma |

Fig. 3.4 Gorlin’s syndrome. People with Gorlin’s syndrome need education about the syndrome, and may need counseling and support because coping with the multiple BCCs and multiple surgeries is often difficult. Genetic counseling is advised for prospective parents, since one parent with Gorlin’s syndrome have 50% chance that their child will also be affected.
The BCNS (NBCCS Gorlin’s syndrome) is a rare, autosomal dominant disorder due to germline mutations of the human patched gene (PTCH). The histologic appearance of the BCCs in BCNS does not differ from those seen in sporadic cases. The diagnosis should be suspected in patients who present with multiple BCCs, especially when these occur at an early age and are located on the trunk. These patients require aggressive approaches to therapy and frequently are disfigured from surgical treatments by the third decade of life. Affected patients have distinct clinical features and predilection for multiple tumors, especially multiple BCCs, usually by age 35.99 Clinical features often include macrocephaly, hypertelorism, bifid ribs, palmar and plantar pitting, osseous cysts (of the mandible), and medulloblastoma (3–5%).99,128

Fig. 3.5 Mandibular cysts of Gorlin’s syndrome. When patients with Gorlin’s syndrome have mandible tumors, they are characterized as keratocystic odontogenic tumors. Above is a Panorex example.

Fig. 3.6 Palmar pits of Gorlin’s syndrome. Palmar and plantar pits appear as punctiform depressions in the skin of palms and soles of feet. These changes are caused by a partial or complete absence of the stratum corneum. They are usually asymmetric, flesh-, pink- or red-colored, and range from 2 to 3 mm in diameter and 1 to 3 mm in depth. In Gorlin’s syndrome, pits appear in 30 to 65% of patients by the age of 10 years and in 85% of patients over the age of 20 years.

Fig. 3.7 Plantar pits of Gorlin’s syndrome.
3.4 Prevention of Basal Cell Carcinoma
The primary approach to the prevention of BCCs is protection from UV radiation exposure. The various techniques to minimize solar exposure are discussed elsewhere. Data on the prevention of BCC through additional drugs or therapies are controversial.129,130,131,132 The results of an 11-month randomized trial of 240 patients with actinically damaged skin suggested that celecoxib may be beneficial for chemoprevention. In this trial, patients treated with celecoxib (200 mg twice daily for 9 months) developed fewer BCCs than patients who were given placebo (adjusted rate ratio 0.40; 95% CI: 0.18–0.93).133 In contrast, a Danish population-based case–control study failed to find an association between the use of celecoxib or other prescription nonsteroidal anti-inflammatory drugs (NSAIDs) and overall risk for BCC.134 Another population-based case–control study did not find an association between the use of any NSAIDs and the overall risk of BCC.135 In subgroup analyses, a modest risk reduction was observed among long-term users of ibuprofen (OR 0.85; 95% CI: 0.77–0.94), and risk was further reduced among mono-users (OR 0.61; 95% CI: 0.48–0.78).135
The Australian Oral Nicotinamide to Reduce Actinic Cancer (ONTRAC) trial preliminarily showed that nicotinamide, a form of vitamin B3, significantly reduced the rates of new cutaneous malignancies in people at high risk of the disease.136 Taken as a twice-daily pill, nicotinamide reduced the incidence of new nonmelanoma skin cancers (NMSCs) by 23%. AK was reduced in the nicotinamide group by 11% at 3 months and by 20% at 9 months of usage. Researchers believe that nicotinamide thus helps replenish cellular energy after sunlight exposure, giving cells the energy boost they need to repair deoxyribonucleic acid (DNA) damage and prevent immune suppression.136
3.5 Clinical Presentation
Approximately 70% of BCCs occur on the face, consistent with the etiologic role of solar radiation. Fifteen percent present on the trunk, and only rarely is BCC diagnosed on areas like the penis, vulva, or perianal skin. Clinically, BCCs appear as pearly and telangiectatic papules or nodules with or without ulceration, or as indurated, erythematous, or ulcerated patches with a discrete papular border, and may be pigmented. BCCs display different morphological growth patterns: superficial or multifocal, nodular, micronodular, infiltrating, sclerosing (sclerodermi-form), or morpheaform.
The diversity in the phenotypic appearance of BCCs indicates that the cell of origin may be a stem or progenitor cell. Moreover, these observations raise the question as to whether BCC is a monoclonal tumor or whether it is the result of field cancerization. Studies investigating clonal patterns of X chromosome inactivation suggest that the majority of BCCs do represent monoclonal tumors and that anatomically distinct BCCs may sometimes share the same cellular origin.137
About 30% of BCCs are superficial BCCs. For unclear reasons, men have a higher incidence of superficial BCC, in particular, than women. Superficial BCCs most commonly occur on the trunk, and typically present as slightly scaly, nonfirm macules, patches, or thin plaques light red to pink in color (![]() Fig. 3.8 and
Fig. 3.8 and ![]() Fig. 3.9). The center of the lesion sometimes exhibits an atrophic appearance and the periphery may be rimmed with fine translucent papules. A shiny quality may be evident when a superficial BCC is illuminated. Occasionally, spotty brown or black pigment as shown in
Fig. 3.9). The center of the lesion sometimes exhibits an atrophic appearance and the periphery may be rimmed with fine translucent papules. A shiny quality may be evident when a superficial BCC is illuminated. Occasionally, spotty brown or black pigment as shown in ![]() Fig. 3.10 is present, which may contribute to confusion with melanoma.138 These lesions are referred to as pigmented BCCs. However, both nodular and superficial BCCs can produce pigment. Superficial BCCs tend to grow slowly, and can vary in size from macules measuring just a few millimeters in diameter to lesions several centimeters in diameter or more if left untreated. Superficial BCCs are usually asymptomatic.138,139,140
Fig. 3.10 is present, which may contribute to confusion with melanoma.138 These lesions are referred to as pigmented BCCs. However, both nodular and superficial BCCs can produce pigment. Superficial BCCs tend to grow slowly, and can vary in size from macules measuring just a few millimeters in diameter to lesions several centimeters in diameter or more if left untreated. Superficial BCCs are usually asymptomatic.138,139,140
Nodular BCCs, which represent about 60% of cases, typically present on the face as a pink or flesh-colored papule. As shown in ![]() Fig. 3.11,
Fig. 3.11, ![]() Fig. 3.12,
Fig. 3.12, ![]() Fig. 3.13,
Fig. 3.13, ![]() Fig. 3.14, these lesions usually have a pearly or translucent quality and a telangiectatic vessel is frequently seen within the papule. Ulceration is frequent, and the term “rodent ulcer” refers to these ulcerated nodular BCCs. Nodular BCCs in particular may resemble adnexal tumors or, in some regions, SCC, as these BCCs demonstrate a variety of types of differentiation including basosquamous or metatypical, cystic, adenoid, pigmented, and infundibulocystic differentiation.141,142
Fig. 3.14, these lesions usually have a pearly or translucent quality and a telangiectatic vessel is frequently seen within the papule. Ulceration is frequent, and the term “rodent ulcer” refers to these ulcerated nodular BCCs. Nodular BCCs in particular may resemble adnexal tumors or, in some regions, SCC, as these BCCs demonstrate a variety of types of differentiation including basosquamous or metatypical, cystic, adenoid, pigmented, and infundibulocystic differentiation.141,142

Fig. 3.8 Superficial basal cell carcinoma (BCC). Superficial BCCs are usually asymptomatic. They present as a flaky erythematous lesions with irregular borders that are slightly elevated.

Fig. 3.9 Superficial basal cell carcinoma (BCC). These often grow slowly but can grow to several centimeters in size if neglected.


Fig. 3.11 Nodular basal cell carcinoma (BCC). The nodular type of basal BCC presents as a pink papule often with pearly borders and fine telangiectasias.

Fig. 3.12 Nodular basal cell carcinoma (BCC).

Fig. 3.13 Ulcerated nodular basal cell carcinoma (BCC). BCC grows over time. With increase in size, it can ulcerate.
Micronodular BCC manifests a plaque-like indurated lesion with a poorly demarcated contour (![]() Fig. 3.15).143,144 Lesions invade deeply in the dermis and so have an increased incidence of recurrence.145,146,147 Micronodular BCC manifests tumor nests with roughly the same shape and contour as nodular BCC, but which are nonetheless smaller and widely dispersed in an often asymmetric distribution extending deeper into the dermis and/or subcutis, as shown in
Fig. 3.15).143,144 Lesions invade deeply in the dermis and so have an increased incidence of recurrence.145,146,147 Micronodular BCC manifests tumor nests with roughly the same shape and contour as nodular BCC, but which are nonetheless smaller and widely dispersed in an often asymmetric distribution extending deeper into the dermis and/or subcutis, as shown in ![]() Fig. 3.16.
Fig. 3.16.
Morpheaform (sclerodermiform) or sclerosing BCCs constitute 5 to 10% of BCCs. These lesions are typically smooth, flesh-colored, or very lightly erythematous papules or plaques that are frequently atrophic resembling scleroderma or “scar-like”; they usually have a firm or indurated quality with ill-defined borders. Some authors group morpheaform, infiltrative, and micronodular as “aggressive-growth” BCC, because they behave similarly.22 Infiltrative and micronodular subtypes are less common than the morpheaform BCC (![]() Fig. 3.17,
Fig. 3.17, ![]() Fig. 3.18,
Fig. 3.18, ![]() Fig. 3.19).
Fig. 3.19).

Fig. 3.14 Pigmented nodular basal cell carcinoma (BCC). BCC may also be pigmented, and sometimes it is easy to confuse it with a malignant melanoma. Pigment may be present in different concentrations in pigmented BCC.

Fig. 3.15 Micronodular basal cell carcinoma (BCC). Micronodular BCCs present as multiple small aggregated nodules. These can invade deeper into the skin and be more aggressive.
Several other BCC subtypes have been described and have a mixed histology and features of more than one histologic sub-type (![]() Fig. 3.20 and
Fig. 3.20 and ![]() Fig. 3.21). BCCs may show a variety of specific cell lineage differentiation features that do not impact prognosis. These include, but are not restricted, to keratotic BCC, infundibulocystic BCC, follicular BCC, which shows collision features with pilomatricoma, pleomorphic BCC, BCC with eccrine differentiation, BCC with sebaceous differentiation, the fibroepithelioma of Pinkus, and the BCC with myoepithelial differentiation. Basosquamous cell carcinoma is an additional sub-type often noted to have a potential for invasion similar to SCC.
Fig. 3.21). BCCs may show a variety of specific cell lineage differentiation features that do not impact prognosis. These include, but are not restricted, to keratotic BCC, infundibulocystic BCC, follicular BCC, which shows collision features with pilomatricoma, pleomorphic BCC, BCC with eccrine differentiation, BCC with sebaceous differentiation, the fibroepithelioma of Pinkus, and the BCC with myoepithelial differentiation. Basosquamous cell carcinoma is an additional sub-type often noted to have a potential for invasion similar to SCC.
Clinicians familiar with the clinical manifestations of BCC are often able to make the diagnosis based upon clinical examination. Dermoscopy, shown in ![]() Fig. 3.22 and
Fig. 3.22 and ![]() Fig. 3.23, is also an important diagnostic tool that every physician who works with skin cancer should be familiar with. Although biopsies are required for a definitive diagnosis, dermoscopy may be used to aid in the clinical evaluation of lesions that are suspicious for BCC.148,149 Common dermatoscopic features of BCC include “arborizing” blood vessels (discrete, thickened, red blood vessels that branch like a tree) and blue-gray ovoid nests. Pigmented BCCs often demonstrate brown leaf-like structures on dermatoscopic examination, which represent heavily pigmented aggregates of tumor cells.149
Fig. 3.23, is also an important diagnostic tool that every physician who works with skin cancer should be familiar with. Although biopsies are required for a definitive diagnosis, dermoscopy may be used to aid in the clinical evaluation of lesions that are suspicious for BCC.148,149 Common dermatoscopic features of BCC include “arborizing” blood vessels (discrete, thickened, red blood vessels that branch like a tree) and blue-gray ovoid nests. Pigmented BCCs often demonstrate brown leaf-like structures on dermatoscopic examination, which represent heavily pigmented aggregates of tumor cells.149
A skin biopsy is usually performed to provide histologic confirmation of the diagnosis. In cases for which the clinical diagnosis of BCC appears certain and the tumor lacks clinical features associated with a high risk for tumor recurrence, clinicians experienced in the diagnosis of BCC sometimes choose to perform the definitive treatment without previous biopsy. However, the decision not to perform a biopsy prior to definitive treatment is not without risk. Because the histologic features of a tumor provide additional information on the risk for tumor recurrence following treatment, not performing a biopsy prior to definitive treatment may result in a failure to detect a tumor with aggressive histologic features that might be best managed with a different approach to therapy. The misdiagnosis of a different tumor as BCC (amelanotic melanoma, Merkel cell carcinoma) is an additional risk of deferring a biopsy, mostly for those who use destruction methods like curettage and electrodesiccation instead of excision biopsy. To reduce the risk for patient mismanagement, one should always perform a biopsy when the diagnosis is uncertain or the lesion exhibits features atypical for BCC, the patient lacks a prior history of BCC, or the lesion exhibits clinical features suggestive of a BCC with a high risk for recurrence.
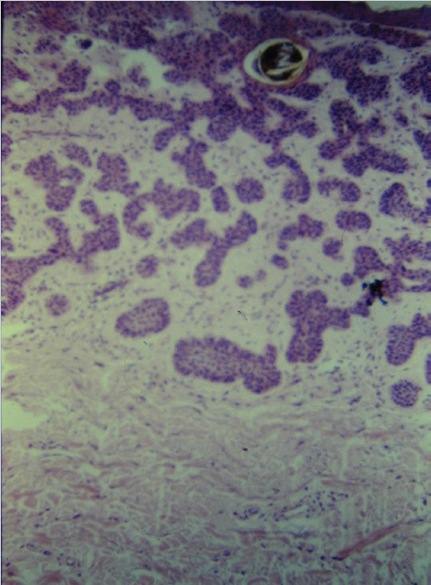
Fig. 3.16 Micronodular basal cell carcinoma (BCC) histopathology. Characteristic feature of small cell nests scattered through the tissue without surrounding stroma.
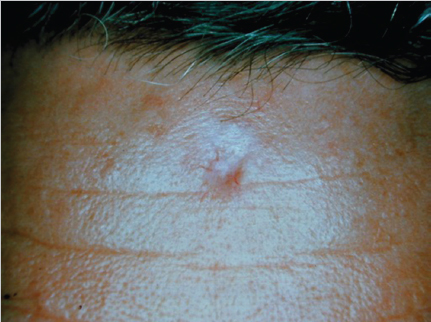
Fig. 3.17 Morpheaform basal cell carcinomas (BCCs) are typically smooth, flesh- or ivory-colored, or very lightly erythematous papules or plaques that are frequently atrophic and sometimes with telangiectasias.

Fig. 3.18 Morpheaform basal cell carcinoma. They usually are firm or indurated with ill-defined borders and may resemble scleroderma.
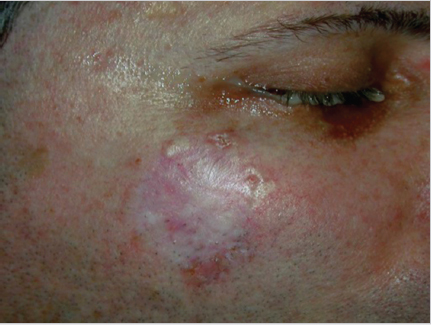
Fig. 3.19 Morpheaform basal cell carcinoma.
Shave biopsies, punch biopsies, and excisional biopsies may all be used for the initial tissue sampling for diagnosis of BCC. Although shave and punch biopsies are frequently performed for diagnosis due to the simplicity of these procedures, clinicians should be aware that biopsies that remove only a portion of the lesion do not provide an accurate assessment of the histologic subtype of a tumor.150,151,152,153 With punch biopsies, an aggressive histologic subtype may be missed in nearly 20% of cases.150,151 A retrospective study in which the majority of biopsy procedures were shave biopsies (230 shave biopsies and 27 punch biopsies) found that an aggressive histologic subtype was missed in 7% of cases.152

Fig. 3.20 (a) Adenoid cystic basal cell carcinoma (BCC). Raised nodule with a thin rim of skin at the periphery. It showed a central ulcer with crusting and irregular rolled borders. (b) BCC with adenoid differentiation of the nose requiring surgical excision.
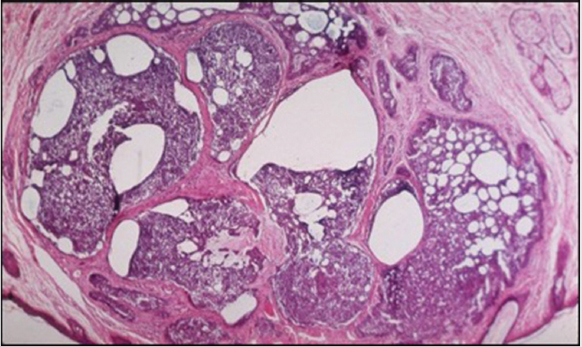
Fig. 3.21 Histopathology adenoid cystic basal cell carcinoma. Histological picture showing a predominant adenoid pattern with thin strands of basaloid cells in a reticulate arrangement, with many tubules and cystically dilated spaces containing mucin.
The differential diagnosis varies with the pathologic sub-type of BCC with nodular, superficial, or morpheaform having various presentations. Early nodular variants with little ulceration clinically may be identical to benign growths such as dermal nevi, small epidermal inclusion cysts, or even sebaceous hyperplasia. A single lesion of molluscum contagiosum has a similar appearance, as does amelanotic melanoma. Larger lesions with central ulceration can appear cup shaped. These can resemble SCC, keratoacanthomas. Superficial BCCs may be confused with inflammatory disorders of the skin such as nummular eczema or psoriasis; therefore, superficial BCC should be considered when a lesion presumed to be inflammatory fails to respond to topical corticosteroids. Morpheaform BCCs frequently appear in or adjacent to a scar or other site of trauma. The induration of the lesion simulates localized scleroderma. Additionally, pigmented nodular or superficial BCCs may resemble melanoma or, less likely, a benign nevus.
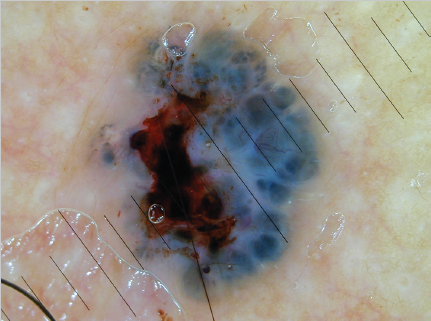
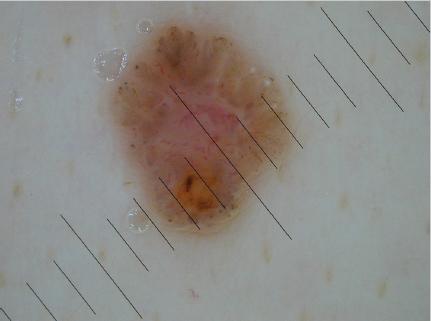
Fig. 3.23 Dermoscopy basal cell carcinoma showing typical absence of pigment network with pinkish color, asymmetrical arborizing vessels, milia formation, and leaflike areas on the periphery of the lesion.
3.6 Biopsy Techniques
Multiple biopsy techniques exist and should be implemented judiciously to each individual patient circumstance. The technique should ideally produce the information necessary for diagnosis and possible staging while maintaining subsequent options for follow-up procedures and long-term care. Disregard to potential follow-up procedures could hinder successful excision, adequate margins, or cosmesis. For example, failure to properly orient the long axis of an incisional or excisional biopsy with respect to future resection could complicate the eventual closure and limit reconstructive options.154
3.6.1 Incisional Biopsy
The incisional biopsy is typically indicated in large lesions in which excision would cause a large defect area, unable to be managed with primary closure. It may also be used in cosmetically sensitive areas before final pathologic diagnosis can be obtained, and a plan for definitive closure/reconstruction can be obtained. The clinician should also attempt to excise a small margin of tissue with the specimen to aid the pathologist in comparing the normal to the abnormal tissue.
3.6.2 Excisional Biopsy
This is the preferred method in relatively small lesions where primary closure and a good cosmetic outcome can be achieved. The advantages of excisional biopsy also include the ability to provide the pathologist with the native architecture, orientation, depth, and appearance of surrounding tissues. In general, margins of 1 to 2 mm are usually sufficient for the primary excision and initial diagnosis, with special attention to excise below the base of the lesion to determine potential Breslow thickness. Furthermore, postoperative margin assessment (POMA) may be requested to ensure adequate excision or diagnose a positive margin that may be missed with traditional pathology sections.155
3.6.3 Punch Biopsy
This is a relatively simple method of obtaining a sample of tissue from a cutaneous lesion. Multiple punches and propriety devices are available including the Tru-Cut needle to obtain a core of tissue from an unknown mass in the skin and/or subcutaneous tissues. The diameter of the punch may be determined by the provider to ensure adequate tissue is sent for pathology.
3.6.4 Shave Biopsy
Shave biopsy is the most common technique used by dermatologists and primary care physicians. The defect site is usually managed by allowing it to heal via secondary intention with adequate scar outcomes. While advantageous in regard to ease of use, cost, and minimal complications, this technique may fail to determine the depth of the tumor margin, and thereby preventing proper staging of the lesion.
3.6.5 Fine-Needle Aspiration Biopsy
This is usually reserved for metastatic lesions that may be easily seen or palpated in the skin or subcutaneous tissue. It is performed by making multiple passes with a hollow-bore needle into the lesion while applying suction on the syringe. The harvested tissue is then placed directly onto a slide for further fixation and analysis.156
3.7 Approach to Treatment
3.7.1 Topical Therapies
Topical therapies include 5-fluorouracil (5-FU) and imiquimod and must be applied for several weeks to maximize potential benefit. In general, both induce mild to moderate inflammatory reactions at the sites of application.157
Topical 5-Fluorouracil
5-FU exerts its affects through interference of DNA synthesis by inhibiting thymidylate synthase, therefore rapidly proliferating cells are most sensitive to its cytotoxic effect. Topical 5-FU is available in a variety of strengths and formulations; the 5% cream or solution is used for the treatment of BCC applied twice daily for at least 3 to 6 weeks; however, treatment may continue until reaching the desired clinical response.157
Treatment with topical 5-FU should be restricted to superficial BCCs in noncritical locations.157 Various relatively small studies have documented cure rates of up to 95% using 5-FU cream in patients with carefully selected superficial BCCs, although lower cure rates are reported by others.157,158 Treatment of nonsuperficial, recurrent, or other high-risk BCCs with 5-FU results in low cure rates and is generally inadvisable.159,160,161 In particular, nodular and aggressive BCCs are generally considered contraindications to topical 5-FU given that superficial treatment may give the false impression of a cure despite persistent dermal disease.
Topical 5-FU causes a brisk inflammatory reaction in the treated sites, which is an indication of activity. Prior to treatment, patients should be thoroughly educated on anticipated side effects, including undesired cosmetic effects, pain, erythema, edema, erosions, and ulceration with potential drainage. Therapy may be discontinued if the inflammation is not tolerated. Alternatively, tolerance may be improved through reduction of drug concentration, application of an emollient or application of an intermediate-potency topical steroid.159,160,161 Special care should be taken when applying 5-FU to areas near the eyes, lips, and nose as well as avoiding intense sun exposure during treatment.
Following discontinuation of topical 5-FU therapy, healing generally takes place over the ensuing 2 weeks or more. The residual erythema and occasional hyperpigmentation usually fade with time. In general, long-term favorable cosmetic results are obtained with observation. Other unusual side effects include persistent telangiectasias, pigmentary changes, and hypertrophic scarring in high-risk areas.
3.7.2 Imiquimod
Imiquimod 5% cream is an immune response modifier (Toll-like receptor 7 agonist) approved for treatment of superficial BCCs in low-risk sites. Imiquimod is thought to promote apoptosis in skin cancer cells by circumventing the antiapoptotic mechanisms deployed by tumor cells or by stimulating monocytes/macrophages and dendritic cells to produce cytokines that stimulate cell-mediated immunity.162,163,164
The efficacy of imiquimod for superficial BCC has been documented in multicenter randomized trials that compared imiquimod 5% cream (applied once daily five or seven times per week for 6 weeks) in a total of 724 patients with superficial BCC.164 Twelve weeks after treatment, the histologic clearance rates for the 5- and 7-day imiquimod treatment groups were 82 and 79%, respectively, compared with 3% in the control group. The severity of erythema, erosion, and scabbing/crusting was associated with higher clearance rates; however, long-term follow-up was not reported. This was corroborated in a randomized trial that assessed the response of superficial BCC to 6 weeks of daily therapy with imiquimod 5% cream.165 Twelve weeks after treatment, histologic clearance rates in the imiquimod and vehicle groups were 80 and 6%, respectively.165
Although imiquimod’s efficacy has been established, clinicians should be aware that the likelihood of treatment success is higher with surgical excision (SE). A trial of 257 patients with superficial BCC and 244 patients with nodular BCC were randomly assigned to treatment with imiquimod 5% cream (once daily for 6 weeks for superficial BCC and once daily for 12 weeks for nodular BCC) or SE with a 4-mm margin found that patients treated with SE were significantly less likely to experience treatment failure or tumor recurrence within 3 years.166 Among the patients with superficial BCC, clinical cure rates from SE and imiquimod were 98 and 85%, respectively.166 Patient satisfaction with the cosmetic appearance of sites of imiquimod treatment and SE was also similar at 6 months and 3 years after treatment.166
The thickness of a superficial BCC may influence the likelihood of response to imiquimod therapy. A retrospective study of 127 biopsy specimens from superficial BCCs that were subsequently treated with imiquimod (applied 5 days per week for 6 weeks) found that while 11 of 19 tumors (58%) > 0.4 mm deep recurred after treatment, none of 108 tumors ≤ 0.4 mm deep recurred (mean follow-up 34 months, range 3–91 months).167 If these findings are supported by future investigations, the depth of superficial BCC may become a consideration in the selection of imiquimod treatment.
The few randomized trials that have evaluated the use of imiquimod as an adjunctive therapy for nodular BCC prior to SE have yielded conflicting findings.168,169 In a randomized trial of 70 patients with nodular BCC on the face, 4 weeks of imiquimod treatment prior to Mohs surgery was associated with reductions in tumor size and surgical defect size. However, a smaller randomized trial failed to find a statistically significant benefit of imiquimod therapy.168 There is also a theoretical concern that pretreatment with imiquimod could contribute to false negative surgical margins by inducing noncontiguous areas of residual tumor.170
In general, imiquimod is used for the treatment of primary superficial BCCs in low-risk sites where recurrence is unlikely to be accompanied by substantial morbidity. Because of concern for consistent patient adherence to the longer treatment period suggested for nodular BCC and the availability of more effective treatment,166 imiquimod is not routinely used for the treatment of nodular BCC. Imiquimod is reserved for the treatment of nonsuperficial BCCs only in those patients who are poor surgical candidates or who have limited life expectancies. The selection of imiquimod over a surgical procedure for superficial BCC usually stems from patient-specific factors such as patient preference to avoid surgery.166
The standard regimen for imiquimod treatment of superficial BCC is application of imiquimod to the BCC once daily 5 days per week for 6 weeks. If the irritation becomes too severe, the patient may take 2 to 3 days off and then resume treatment. Local skin irritation is an expected side effect of imiquimod therapy. Patients may experience itching, weeping, redness, soreness, bleeding, and/or pain within the treated area.166 In addition, hypopigmentation may develop after therapy.166,171
3.8 Photodynamic Therapy
Photodynamic therapy (PDT) utilizes both light and porphyrins to cause tumor destruction. PDT is applied to the lesion, which results in a higher concentration of the porphyrins within the cancerous cells, and the ability to focus light on the involved area. Although PDT has been approved for the treatment of BCC in many European countries, U.S. Food and Drug Administration (FDA) approval has not been granted for the treatment of BCC.
To perform PDT, a photosensitizing porphyrin such as 5-aminolevulinic acid (ALA) or methyl aminolevulinate (MAL) is applied topically to the lesion.172,173 Although the porphyrin porfimer can be administered systemically, systemic therapy can be associated with prolonged photosensitivity.172,173 Several hours after topical application of the porphyrin, the area is exposed to visible light. The light penetrates the skin and is selectively absorbed by the photosensitizer, which generates reactive oxygen species. This in turn can cause lipid peroxidation, protein crosslinking, increased membrane permeability, and ultimately cell death. In addition to direct effects on tumor cells, PDT can damage blood vessels, resulting in impaired blood flow, and can stimulate a vigorous local inflammatory reaction that may contribute to tumor destruction.174
Response to PDT has been variable. Superficial lesions appear to be most responsive to therapy with response rates ranging from 72 to 100%.175,176,177,178 Three randomized controlled trials (RCTs) with long-term follow-up have compared various PDT protocols against simple SE for sBCC and primary nBCC. All demonstrated statistically superior clearance rates with SE over PDT.179 Side effects from topical PDT include photosensitivity, pain, erythema, edema, ulceration, and temporary pigmentary change at the treated site. Healing is usually complete within 2 weeks and there is low probability of scarring.
3.9 Radiation Therapy
Radiation therapy (RT) is an option for the treatment of BCCs in patients who are poor candidates for surgical intervention or in patients with positive surgical margins. RT is usually administered in a fractionated schedule to limit treatment-related side effects; however, it requires multiple sessions and strict compliance (![]() Table 3.2). RT results in relative sparing of cosmetically and functional tissues, its noninvasive and painless nature, and its utility for many patients who are not candidates for surgical intervention or for whom it is difficult to attain histologic clearance. Unlike SE, RT does not provide histologic control of the tumor margin. Most large series report overall 5-year cure rates of 91 to 93% for previously untreated BCCs, with rates as high as 96% for smaller BCCs at low risk for recurrence.180,181,182 For patients with recurrent BCCs, the reported cure rates are generally reported between 86 and 91%.180,181,182,183 BCCs that recur following RT may behave more aggressively than those recurring after surgical procedures, with higher rates of second recurrence and distant metastasis.184
Table 3.2). RT results in relative sparing of cosmetically and functional tissues, its noninvasive and painless nature, and its utility for many patients who are not candidates for surgical intervention or for whom it is difficult to attain histologic clearance. Unlike SE, RT does not provide histologic control of the tumor margin. Most large series report overall 5-year cure rates of 91 to 93% for previously untreated BCCs, with rates as high as 96% for smaller BCCs at low risk for recurrence.180,181,182 For patients with recurrent BCCs, the reported cure rates are generally reported between 86 and 91%.180,181,182,183 BCCs that recur following RT may behave more aggressively than those recurring after surgical procedures, with higher rates of second recurrence and distant metastasis.184
Short-term cutaneous side effects of RT include erythema and edema, scaling, vesicles, bullae, erosions, ulceration, pain, and occasionally infection. Healing generally occurs within 3 to 4 weeks following the final treatment, but symptoms may persist for months in severe cases. Other less common short-term side effects include a “comedo reaction,” which is a benign condition characterized by the appearance of large, open come-dones at the periphery of the treated areas.
Table 3.2 Radiation therapy regimens for basal cell carcinoma
Tumor diameter | Margin | Electron beam radiation therapy |
< 2 cm | 1–1.5 cm | 64 Gy in 32 fractions over 6–6.4 wk |
|
| 55 Gy in 20 fractions over 4 wk |
|
| 50 Gy in 15 fractions over 3 wk |
|
| 35 Gy in 5 fractions over 5 d |
> 2 cm | 1.5–2 cm | 66 Gy in 33 fractions over 6–6.6 wk |
|
| 55 Gy in 20 fractions over 4 wk |
Postoperative adjuvant Therapy |
| 50 Gy in 20 fractions over 4 wk |
|
| 60 Gy in 30 fractions over 6 wk |
Delayed effects of radiation within the treatment field include permanent alopecia that usually occurs within the treatment field. Patients should be advised of this prior to treatment, and pretreatment counseling is essential. Chronic radiation dermatitis generally appears months to years following therapy and is characterized by permanently mottled areas of hypopigmentation and hyperpigmentation, a dry, hyperkeratotic, atrophic, shiny epidermis, telangiectasias, and dermal fibrosis. Severe dermal and subcutaneous fibrosis is an uncommon consequence of RT for cutaneous malignancies.
Delayed radiation necrosis may develop months to years following RT, and is marked by spontaneous breakdown of the skin within the treatment field, with erythema, erosions or ulcerations, crusting, and discomfort. Radiation necrosis is usually precipitated by trauma, infection, or exposure to cold or sunshine, and is secondary to poor vascularity and atrophy of the previously irradiated area. Irradiation of cartilaginous and bony structures such as the ear and nose may result in chondroradionecrosis or osteoradionecrosis, although this is uncommon using modern techniques.185
Risk factors for secondary cancers after RT include higher radiation doses, larger radiation fields, sun-exposed sites, fair skin, and early age of radiation exposure. Increased fractionation with a smaller dose per fraction reduces this risk. Although some investigators think that the risk of radiation-induced cutaneous malignancy is much smaller using modern treatment protocols, RT continues to be avoided in young people and in those with genetic susceptibility to radiation-induced malignancies.186 Incidental radiation exposure to other tissues can also result in delayed complications, such as cataracts, infertility, and thyroid cancer. These are uncommon events that should be avoided with proper shielding during therapy.
3.10 Intralesional Therapy
Intralesional therapies (interferons, 5-FU, or bleomycin) are used infrequently for the management of BCC; however, these therapies may have a place in modern regimens.187,188 A systematic review of open label studies, case series, and the few randomized trials that have investigated the efficacy of intralesional interferon for BCC found overall cure rates for interferon beta, interferon alfa-2a, and interferon alfa-2b of 63, 68, and 76%, respectively.187 Data are limited on the use of intralesional 5-FU and bleomycin; however, the results of a few case reports and small case series suggest that these therapies may be highly effective for BCC.189,190,191,192 Adverse effects of intralesional interferon, 5-FU, and bleomycin include local pain, erythema, necrosis, and ulceration.187 Systemic side effects are less likely with intralesional injection than with systemic administration, but may also occur. Risks of interferon therapy include fever, malaise, headaches, myalgias, cytopenia, hepatotoxicity, and nephrotoxicity. Pulmonary toxicity, cutaneous sclerosis, and Raynaud phenomenon have been associated with bleomycin. Gastrointestinal distress and cytopenias are potential adverse effects of 5-FU. Evidence is limited on the long-term efficacy of intralesional therapies for BCC.
3.11 Targeted Therapy for BCC Including LABCC and MBCC and Hedgehog Pathway
BCCs that are extensive or invade below the dermis and potentially vital structures are difficult to surgically clear without significant morbidity. Many of these may become locally advanced or metastasize. Although low, estimates of the metastatic rate of BCC ranged from 0.0029 to 0.55%.193 In another report, the population-based case mortality rate from BCC was approximately 0.05%.194 Men develop metastatic disease more frequently than women, although the reason for this is unknown. Metastatic lesions usually result from primary, deeply invasive, or large lesions with an area of greater than 10 cm.2,193 The most common sites for metastasis include the regional lymph nodes, lungs, bones, skin, and liver.195
BCCs that metastasize to either local or distant lymph nodes or distant organs would best be addressed through systemic therapy. Together, these locally advanced or metastatic BCCs comprise a disease group termed “locally advanced BCCs” (LABCCs). While accurate estimates of the incidence of LABCCs are difficult to obtain, in part due to the lack of widespread use of a staging system by dermatologists and lack of uniform reporting requirements for NMSCs, LABCCs are thought to represent roughly 1 to 10% of all BCCs, with metastatic BCCs accounting for 0.0028 to 0.5%.196,197,198 From our clinical experience, patients presenting with LABCCs appear to fall into two categories: those who present with LABCC due to delay in accessing medical attention or those who have BCCs that are intrinsically aggressive, are refractory, or recur after treatment. Included in this group are those patients with chronic immunosuppression following organ transplant and some patients with Gorlin’s syndrome. Therapeutic options for such patients are limited.199,200
The Hedgehog pathway was initially identified as a critical developmental regulator of embryonic segment polarity in Drosophila in 1980.201 This and related developmental work in fly body patterning was recognized by the Nobel Prize in Physiology and Medicine in 1995. Vertebrate homologs of the Drosophila Hedgehog ligand were first reported in 1993, and definition of central components of the mammalian signaling pathway followed in the late 1990s and early 2000s.202 The first definitive linkage of mutation in this pathway to cancer, that is, to development of BCC, was made in 1996.101,203
Hedgehog signaling regulates embryonic development ensuring that tissues reach their correct location, size, and cellular content. The Hedgehog pathway normally remains inactive in adult tissues; however, reactivation of this pathway results in malignant transformation and tumorigenesis.204,205 More than 90% of all BCCs have identified abnormal Hedgehog pathway signaling. There are two classic mechanisms of Hedgehog pathway reactivation: mutation-driven signaling (ligand independent) and abnormal signaling in the tumor microenvironment (ligand dependent).94 In mutation-driven signaling, tumor cells harbor mutations in key components of the Hedgehog pathway allowing for independent activation of the biomolecular system and subsequent stimulation of unregulated proliferation.206 In ligand-dependent activation, tumor cells overexpress Hedgehog ligands that activate surrounding stromal cells leading to uncontrolled growth.207 Mutations in two major receptor proteins, Patched-1 (PTCH1) and Smoothened (SMO), may result in abnormal activation of the Hedgehog pathway and are the focus of proposed interventions.
As shown in ![]() Fig. 3.24, Hedgehog pathway activation occurs via binding of an extracellular Hedgehog ligand (Shh) to PTCH1, a transmembrane receptor. Once bound, PTCH1 is internalized and degraded, allowing for release of a the transmembrane protein SMO from the inhibitory effect of PTCH1.111 SMO can then move from the intracellular compartment to the cell membrane of the cilium and activate the GLI family of transcription factors. Activated GLI factors enter the nucleus and initiate the transcription of target genes.111 The majority of sporadic BCCs contain mutations that result in inactivation of PTCH1, with subsequent constitutional activation of SMO.208 Inhibition of SMO activation, either through appropriate PTCH hindrance or through new SMO inhibitors such as vismodegib (Erivedge, Genentech), prevents unregulated proliferation.
Fig. 3.24, Hedgehog pathway activation occurs via binding of an extracellular Hedgehog ligand (Shh) to PTCH1, a transmembrane receptor. Once bound, PTCH1 is internalized and degraded, allowing for release of a the transmembrane protein SMO from the inhibitory effect of PTCH1.111 SMO can then move from the intracellular compartment to the cell membrane of the cilium and activate the GLI family of transcription factors. Activated GLI factors enter the nucleus and initiate the transcription of target genes.111 The majority of sporadic BCCs contain mutations that result in inactivation of PTCH1, with subsequent constitutional activation of SMO.208 Inhibition of SMO activation, either through appropriate PTCH hindrance or through new SMO inhibitors such as vismodegib (Erivedge, Genentech), prevents unregulated proliferation.
Basal cell carcinoma (BCC), medulloblastoma, rhabdomyosarcoma, and other human tumors are associated with mutations that activate the proto-oncogene Smoothened (SMO) or that inactivate the tumor suppressor Patched (PTCH). Smoothened and Patched mediate the cellular response to the Hedgehog (Hh) secreted protein signal, and oncogenic mutations affecting these proteins cause excess activity of the Hh response pathway.
The story of how the first inhibitor of the Hh pathway, cyclopamine, was discovered is one of the most fascinating in biomedicine. In the late 1950s, pregnant ewes were found to produce one-eyed offspring, or extreme holoprosencephaly199,209 (![]() Fig. 3.25).
Fig. 3.25).
In the 1970s, the active agent inducing these changes, cyclopamine, was isolated and its structural formula identified. Subsequent studies in the 1990s in chick embryos demonstrated cyclopamine’s ability to induce holoprosencephaly and to bind the transmembrane protein, Smoothened.210 Subsequently, a number of analogues were developed by modifications to cyclopamine to improve solubility, and oral bioavailability. Collectively, these analogues are called Smoothened inhibitors (SIs), due to their targeting of the Smoothened protein.
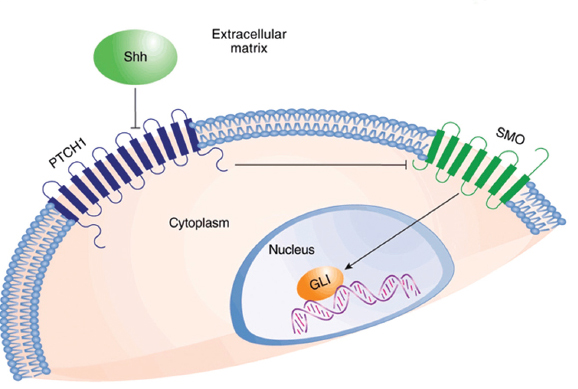
Fig. 3.24 Simplified schematic of common mutations in the Hedgehog signaling pathway leading to basal cell carcinoma from pathway activation. (Reprinted with permission from Sheridan C. Genentech obtains proof of concept for hedgehog inhibition. Nat Biotechnol 2009;27:968–969.)

Fig. 3.25 In the decade after World War II, Idaho farmers noticed that a random batch of their lambs was being born with strange birth defects. The creatures had underdeveloped brains and a single eye planted, Cyclops-like, in the middle of their foreheads. In 1957, they called in scientists that worked for 11 years to solve the mystery: corn lilies. When the animals moved to higher ground during droughts, they snacked on the flowers. The lilies, it turned out, contained a poison, later dubbed cyclopamine that stunted developing lamb embryos. The adult mothers remained unharmed. The case of the cyclopamine and the one-eyed Idaho lambs remained a freakish chemistry footnote for the next three decades.
In 2000, Taipale et al showed that cyclopamine inhibits the Hh response and was a potential “mechanism-based” therapeutic agent for treatment of some tumors. They showed that cyclopamine or synthetic derivatives with improved potency, block activation of the Hh response pathway, and abnormal cell growth associated with both types of oncogenic mutation. Their results also indicated that cyclopamine could act by influencing the balance between active and inactive forms of SMO.211,212,213
This discovery, together with rapidly accumulating evidence implicating the Hh pathway in oncogenesis, led to focused efforts by multiple biotechnology and pharmaceutical companies to develop cyclopamine derivatives with improved pharmacologic properties or to develop agents that effectively outcompeted cyclopamine for binding to the critical cell-surface activator of Hh signaling, the 7-transmembrane G-protein-coupled–like receptor, SMO. Vismodegib is a member of this class: structurally unrelated to cyclopamine but able to bind with high affinity and specificity to SMO, leading to potent suppression of Hh signaling in reporter systems and in a preclinical model of Hh-dependent disease.214 An Investigational New Drug application for vismodegib was filled with the FDA in September 2006, leading to launch of a first-in-human phase I clinical trial at three U.S. sites in January 2007.
Multiple orally available smoothness inhibitors are currently in human clinical trials against BCCs. The first and only U.S. FDA-approved SI for advanced BCCs (aBCCs) to date is vismodegib, which became commercially available in 2012. The phase II study with 96 aBCC patients leading to FDA approval demonstrated an independently assessed response rate of 30% in patients with metastatic BCC and 43% response rate in LABCC.215 A subsequent study of 119 aBCC patients showed similar findings.216 The availability of vismodegib as highly targeted therapy for aBCCs is one of the greatest success stories in translational medicine.
Initial investigation of Vismodegib documented its therapeutic effects in both in vitro studies with downregulation of GLI1 by approximately 90% compared to controls and in ex vivo analysis with reported downregulation of GLI1 by greater than 50% in skin biopsy specimens excised from treated patients.214,217 A phase 1 trial with vismodegib included 68 patients with solid tumors, of which 33 had aBCC, 8 had pancreatic cancer, 1 had medulloblastoma, in addition to 17 other types. The overall rate of complete or partial response was 58% with specific response of 50% in patients with metastatic BCC and 60% in patients with LABCC.217 Despite vast heterogeneity with respect to tumor histology, patient characteristics, and dosing concentrations, vismodegib was generally well tolerated with 8.8% experiencing a grade 4 event (hyponatremia, fatigue, pyelonephritis, presyn-cope, resectable pancreatic adenocarcinoma, and paranoia with hyperglycemia), and 27.9% of patients experienced a grade 3 event (hyponatremia [10.3%], abdominal pain [7.4%], and fatigue [5.9%]).
A multicenter, nonrandomized phase 2 clinical trial of vismodegib in 104 patients was conducted from February 2009 through November 2010.215 Of the 33 patients with metastatic BCC, 10 (30%) had a response as judged by independent review, and 15 (45%) had a response as judged by site investigators. In the 63 patients with LABCC, 38 (60%) had at least a partial response as judged by site investigators, with 13 (21%) judged to have a complete response with verification established by the absence of residual disease on biopsy.218
An additional phase 2 trial was conducted in 41 patients with basal cell nevus syndrome (BCNS).219 Vismodegib was associated with a decrease in the number of new and existing surgically eligible BCCs with surgically eligible BCCs occurring at a rate of 2 per year in the vismodegib group compared with 29 per year in the control group (p < 0.001). There was also a significantly greater decrease in the size of existing surgically eligible BCCs in patients receiving vismodegib (65% in the vismodegib group vs. 11% in the control group; p = 0.003).218
Current research and clinical trials focusing on the administration of synthetic SMO inhibitors, or Hh pathway inhibitors, for patients with locally advanced and metastatic basal cell carcinoma (MBCC) are ongoing.220,221 Clinical trials have shown exceptional decrements in tumor burden as well as resolution of metastatic disease with the drug as the sole treatment modality, thus reducing the need for SE and associated morbidity and mortality.218 Furthermore, recent case reports have documented the use of vismodegib as a potential neoadjuvant therapy prior to surgical or radiotherapeutic intervention.216,222,223
Although ongoing clinical trials for topical and systemic therapies are currently pending, vismodegib remains the only FDA-approved Hh pathway inhibitor approved for the treatment of metastatic and LABCC.224
More recently, evolving treatment protocols have led to novel algorithms of treatment under clinical trial settings. Targeted therapy with Hh inhibitors including vismodegib has served as both a viable alternative and adjunct to SE alone in the author’s practice. As example we present data of our first consecutive series of 20 patients initially treated from April 2012 to June 2013. All adult patients with locally advanced basal cell carcinoma (LABCC) and/or recurring or MBCC who were not candidates for surgery or RT (due to clinical morbidities or patient’s refusal of surgery/RT) received vismodegib 150 mg once a day until disease progression, unacceptable side effects, or discontinuation of treatment at patients’ request. The peak plasma concentration of vismodegib is reached 48 hours after oral administration and maintained for 72 hours, formulating the currently recommending schedule of 150-mg PO daily.217,225 LABCC was defined as at least one lesion 20 mm or more in areas of limited tissue availability (eyelid, ear, nasal ala, etc.); patients that had recurrence after two or more surgical procedures and curative resection was unlikely and surgery was expected to result in substantial morbidity and/or deformity.
Response was defined as a decrease of ≥ 30% in the externally visible or radiographic dimension or complete resolution of ulceration if present at baseline. Radiographic imaging was obtained for all patients with MBCC and for patients with LABCC who had radiographically measurable disease. Objective response of vismodegib on tumor regression and prevention of disease progression was visually and clinically appreciable in almost all treated patients. As of the data-cutoff point 13/20 (65%) patients had complete response (defined as the absence of residual BCC on assessment of a biopsy specimen) and 7/20 (35%) patients had partial response. As of the data-cutoff point, 13 of the 13 patients who had a complete response did not have disease progression (![]() Fig. 3.26 and
Fig. 3.26 and ![]() Fig. 3.27). One patient was excluded from treatment on his request due to unacceptable side effects (loss of taste and muscle cramps). Most common side effects were loss of taste (100%), muscle spasms (80%), hair loss (50%), weight loss (30%), and fatigue (10%). Once treatment stopped, the side effects subsided. Surgery was performed in the seven patients who had partial response. Minimal residual tumor was identified in five of them and no residual tumor was found in two of the patients.
Fig. 3.27). One patient was excluded from treatment on his request due to unacceptable side effects (loss of taste and muscle cramps). Most common side effects were loss of taste (100%), muscle spasms (80%), hair loss (50%), weight loss (30%), and fatigue (10%). Once treatment stopped, the side effects subsided. Surgery was performed in the seven patients who had partial response. Minimal residual tumor was identified in five of them and no residual tumor was found in two of the patients.
In ![]() Fig. 3.27a, marked resolution of the tumor with reduction in vertical height and surrounding erythema was evident by day 30 of treatment. By day 120, there were no palpable lesions and the surrounding erythema and induration associated with the metastatic lesion had been greatly diminished. Radiographically, the patient had exceptional regression of tumor burden matching the clinical picture. The chemotherapeutic agent not only benefited the cutaneous manifestations of disease, but also had a profound effect on systemic metastases as shown in
Fig. 3.27a, marked resolution of the tumor with reduction in vertical height and surrounding erythema was evident by day 30 of treatment. By day 120, there were no palpable lesions and the surrounding erythema and induration associated with the metastatic lesion had been greatly diminished. Radiographically, the patient had exceptional regression of tumor burden matching the clinical picture. The chemotherapeutic agent not only benefited the cutaneous manifestations of disease, but also had a profound effect on systemic metastases as shown in ![]() Fig. 3.27b. By day 120, the patient with cutaneous lesions (
Fig. 3.27b. By day 120, the patient with cutaneous lesions (![]() Fig. 3.27) had radiographic evidence of complete resolution of pulmonary metastases.
Fig. 3.27) had radiographic evidence of complete resolution of pulmonary metastases.
In this series of 20 consecutive patients, vismodegib showed encouraging results with objective response rate superior to 90% and provided substantial clinical benefit for the selected patients. However, treatment patterns, clinical outcomes, health care resource use, and definitions of advanced and complex/difficult-to-treat disease are not uniformly adopted in the literature and clinical practice.
Itraconazole, an antifungal agent, has also been identified as a potent inhibitor of the Hh signaling pathway.226 In a phase II trial including 29 patients with sporadic BCC > 4 mm, 15 patients were treated with 200 mg twice daily for 4 weeks prior to surgery and 4 patients with 100 mg twice daily for 1 to 4 months (mean 2.3 months).227 Itraconazole reduced tumor size by 24% and promoted re-epithelialization in 8 patients with a total of 57 tumors. Further data from more robust trials are pending; however, itraconazole may play a role in vismodegib-resistant subjects or in BCC prevention.
3.12 Surgical Management
Surgical options for BCCs at low risk for recurrence include electrodesiccation and curettage (ED&C), conventional SE, and cryosurgery. Cryosurgery is infrequently used for this indication and ED&C is mainly used by dermatologists and primary care physicians.

Related posts:
 Mohs Micrographic Surgery’s Role in the Treatment of Skin Cancer
Mohs Micrographic Surgery’s Role in the Treatment of Skin Cancer
 Common Reconstructive Techniques after Facial Skin Cancer Excision
Common Reconstructive Techniques after Facial Skin Cancer Excision
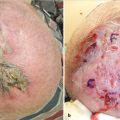 Clinical Detection of Skin Cancer
Clinical Detection of Skin Cancer
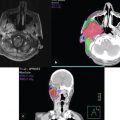 Role of Radiotherapy in the Treatment of Skin Malignancies
Role of Radiotherapy in the Treatment of Skin Malignancies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


