4 Surgical Treatment of Cutaneous Melanoma Melanoma is currently the fifth most common cancer in the United States, and its incidence is continuing to increase. In 2017, over 87,000 new cases of invasive melanoma will be diagnosed, accounting for about 4.5% of new cancer cases in the United States. Although the 5-year survival rate continues to improve, and is now estimated at 92% for all stages at presentation, about 10,000 deaths from this disease now occur in the United States annually.1 Because of its relatively early age of onset, melanoma is one of the most devastating malignant diseases in terms of the years of potential life lost per death.2 Both environmental and genetic factors increase an individual’s risk for developing melanoma ( Any patient who presents with a new or abnormal pigmented skin lesion, with increasing size, change in color, or developing irregular borders, should be considered for a biopsy for definitive diagnosis. The approach to biopsy for a suspicious cutaneous lesion often varies depending on the location of the lesion and the preference and training of the physician performing the biopsy. The gold standard for tissue diagnosis when melanoma is suspected is excisional biopsy with a 1 mm to 2 mm margin of normal skin, including some subcutaneous fat (see Chapter 2). This may not be feasible in all cases due to the location of the lesion, and often is more than the minimum necessary for the diagnosis of a benign lesion.8 Several other biopsy approaches are reasonable to achieve adequate tissue to allow the pathologist to make a diagnosis and assess all relevant histologic features. These techniques include superficial shave biopsy, deep scallop shave biopsy, punch biopsy, incisional biopsy, and the aforementioned excisional biopsy. When any form of partial biopsy is performed, the biopsy should focus on obtaining a sample of the most elevated portion of the lesion to provide the best estimate of tumor thickness. It is ideal to also include a portion of normal skin in the biopsy; however, the main goal should be to obtain the most suspicious and elevated portion of the lesion in the specimen. For lesions that are large or in cosmetically sensitive areas, a punch biopsy that obtains a full-thickness sample is often the best initial diagnostic approach. If a partial biopsy is performed and a portion of the suspicious lesion remains, indicating this on the pathology request helps make the pathologist aware that the lesion was not removed in its entirety, aiding in the diagnostic process. If a lesion is suspected to be melanoma, cryosurgery and electrodessication should not be performed given they can distort normal tissue planes and do not allow for an adequate histologic evaluation. Partial-thickness shave biopsy of pigmented lesions remains controversial. One of the biggest criticisms of shave biopsy is that partial sampling does not assess the true thickness of a melanoma, if present. Thus, inaccurate microstaging and inappropriate treatment decisions may result.9,10 A multi-institution, retrospective study evaluated over 600 patients diagnosed via shave biopsy with a melanoma that had a Breslow thickness ≤ 2 mm to determine the accuracy of microstaging in these patients. The results demonstrated that the treatment recommendations for excision margin width or sentinel lymph node biopsy changed based on more extensive residual melanoma in the re-excision specimen in only 2% and 1.3% of patients, respectively.11 This study supports the use of shave biopsy as a diagnostic tool for patients with pigmented lesions, especially when they are not considered highly suspicious for melanoma. In essence, it is better to have a partial biopsy of a melanoma than no biopsy at all. Table 4.1 Risk factors influencing the development of cutaneous melanoma
4.1 Epidemiology
![]() Table 4.1). Caucasian race and fair complexion predispose an individual to developing melanoma, as do mutations in several known—and likely multiple as yet unknown—melanoma susceptibility genes.3,4 Melanoma affects a broad age range. According to recent cancer statistics, the peak incidence is between the ages of 55 and 74 years, with a median age at time of diagnosis of 64 years.5 Three-quarters of all cases will occur before age 70, and approximately 20% occur in individuals under 40 years of age. Environmental exposure in the form of ultraviolent radiation is the most well-studied and modifiable etiologic factor in the development of melanoma. Intermittent, high-intensity exposure (e.g., blistering sunburns) contributes most dramatically to the development of melanoma. Dark-skinned individuals may be less likely than fair-skinned individuals to develop melanoma due to the protective effect of eumelanin. Even in individuals with a genetic predisposition, exposure to ultraviolet radiation is the primary factor determining whether an at-risk person actually develops melanoma.6,7
Table 4.1). Caucasian race and fair complexion predispose an individual to developing melanoma, as do mutations in several known—and likely multiple as yet unknown—melanoma susceptibility genes.3,4 Melanoma affects a broad age range. According to recent cancer statistics, the peak incidence is between the ages of 55 and 74 years, with a median age at time of diagnosis of 64 years.5 Three-quarters of all cases will occur before age 70, and approximately 20% occur in individuals under 40 years of age. Environmental exposure in the form of ultraviolent radiation is the most well-studied and modifiable etiologic factor in the development of melanoma. Intermittent, high-intensity exposure (e.g., blistering sunburns) contributes most dramatically to the development of melanoma. Dark-skinned individuals may be less likely than fair-skinned individuals to develop melanoma due to the protective effect of eumelanin. Even in individuals with a genetic predisposition, exposure to ultraviolet radiation is the primary factor determining whether an at-risk person actually develops melanoma.6,7
4.2 Biopsy Techniques and Orientation of Incision
Demographic risk factors | |
Race | Caucasian > Hispanic > American Indian/Alaska Native > Asian Pacific Islander > Black |
Gender | Male > Female |
Age | Median age at diagnosis 62 years old |
Phenotypic features | Light hair, light eyes, fair skin, multiple atypical nevi |
Environmental risk factors | |
Ultraviolet light | Intermittent/intense and chronic cumulative exposure |
Cancer history | Melanoma or nonmelanoma skin cancer: threefold relative risk Childhood history of sarcoma, lymphoma, leukemia, or central nervous system: 2.5-fold risk |
Immunosuppression | Threefold to fourfold risk after organ transplantation |
Socioeconomic status | More likely to have thicker and more aggressive tumors if lower socioeconomic status |
Genetic risk factors | |
Family history of melanoma | 1.7-fold increased relative risk |
CDKN2A, CDK4 mutations | Familial melanoma syndrome |
Source: Adapted from Sondak VK, Jensen EJ, Margolin KA. Melanoma and other cutaneous malignancies. In: Norton JA, Barie PS, Bollinger RR, et al, eds. 2nd ed. Surgery: Basic Science and Clinical Evidence. York, NY: Springer; 2008.
4.3 Margins of Excision
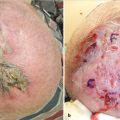
The goal of the initial biopsy is to obtain a diagnosis, but once a diagnosis of melanoma is made, the emphasis shifts to determining the appropriate margins of excision around the biopsy site or residual pigmented lesion. Adequate margins may reduce the risk of local recurrence, while insufficient margins may predispose the patient to a recurrence of disease. A histologically negative margin is always the goal of surgery on the primary melanoma site. The chosen margin should be measured from the edges of the previous biopsy site or any residual pigmentation. Of note, these are “radial” margins, meaning measured in all directions on the skin except downward. The deep margin is the investing fascia of the muscle, which may or may not be included en bloc at the surgeon’s discretion. The recommendation for how much of a margin of normal tissue is taken beyond the biopsy site is based on the Breslow thickness of the melanoma as well as the anatomic location of the tumor. Different margin widths may be recommended for melanomas that are in situ, thin (≤ 1 mm), intermediate (1.1–2 mm or 2.1–4 mm), or thick (> 4 mm).
4.3.1 Melanoma in situ
Melanoma in situ is a lesion with a capacity to progress to invasive melanoma and, like invasive melanoma, should be resected with a measured margin of normal skin and with the goal of achieving histologically negative margins. Recommendations from the National Comprehensive Cancer Network (NCCN) are for a 0.5 cm to 1 cm margin; however, no randomized, prospective study has been conducted to definitively answer what margin is truly necessary.12 In the absence of prospective data, we take into account the location of the lesion and the presence of any residual pigmentation (which might signal the presence of invasive melanoma) in deciding on an appropriate margin of excision for melanoma in situ. In areas with greater tissue laxity, a 1 cm margin may be more easily obtained and is therefore favored, especially when residual pigmentation is present. Conversely, in cosmetically sensitive areas such as the face, neck, hands, and feet, or in locations where the skin is under greater tension, a margin of 0.5 cm is more likely to be used.
4.3.2 Invasive Melanoma: Thin and Intermediate Thickness
The recommended margins of excision for invasive melanoma range from 1 to 2 cm based on the Breslow thickness of the primary tumor. Current NCCN recommendations call for a 1-cm margin for thin melanoma (T1), 1 cm to 2 cm for intermediate melanoma (T2–T3), and 2 cm for thick melanoma (T4).12 The World Health Organization (WHO) trial, two Swedish Melanoma Study Group Trials, and the Intergroup Melanoma Trial have provided prospective randomized trial data that serve as the basis for current margin width recommendations (![]() Table 4.2). In the WHO trial, over 600 patients with melanomas ≤ 2mm in thickness were randomized to either a 1 cm or 3 cm margin. There was no statistical difference between the study arms in local recurrence, disease-free survival, or overall survival.13 This trial concluded 3 cm margins were not necessary for melanomas 2 mm or less in thickness. In particular, the risk of any form of recurrence was very low for melanomas 1-mm thick or thinner even with a 1 cm margin. Hence, a 1 cm margin has become the worldwide standard for excision of invasive melanomas up to 1 mm in thickness, regardless of location of the tumor.
Table 4.2). In the WHO trial, over 600 patients with melanomas ≤ 2mm in thickness were randomized to either a 1 cm or 3 cm margin. There was no statistical difference between the study arms in local recurrence, disease-free survival, or overall survival.13 This trial concluded 3 cm margins were not necessary for melanomas 2 mm or less in thickness. In particular, the risk of any form of recurrence was very low for melanomas 1-mm thick or thinner even with a 1 cm margin. Hence, a 1 cm margin has become the worldwide standard for excision of invasive melanomas up to 1 mm in thickness, regardless of location of the tumor.
The first Swedish Melanoma Study Group Trial evaluated 989 patients with melanomas 0.8 mm to 2 mm in thickness that were resected with either a 2 cm or 5 cm margin. The study evaluated overall and recurrence-free survival and found no statistically significant difference between the arms.14 The authors concluded that 5 cm margins were not necessary for a melanoma 2 mm or less in thickness.
Melanoma thickness | Recommendations regarding margin | Recommendations regarding sentinel lymph node biopsy |
Melanoma in situ | 0.5–1 cm | Not recommended |
< 0.76 mm | 1 cm | Not recommended |
0.76–0.99 mm (no ulceration and mitotic rate < 1/mm2) | 1 cm | SLNB in younger, otherwise healthy patients; nodal observation in older or infirm patients |
0.76–0.99 mm (ulcerated or mitotic rate ≥ 1/mm2) | 1 cm | SLNB unless contraindicated |
≥ 1.0 mm | 1–2 cm for 1.0–2.0 mm; 2 cm for > 2.0 mm | SLNB unless contraindicated |
Abbreviation: SLNB, sentinel lymph node biopsy.
The Intergroup Melanoma Trial evaluated outcomes when margins of 2 cm versus 4 cm were used for patients with a melanoma between 1 mm and 4 mm in thickness. The study evaluated local recurrence as the site of first relapse and at any time, and found no significant difference in outcomes between the two arms. The local recurrence rates as first relapse and at any time for a 2 cm margin (0.4 and 2.1%, respectively) were not significantly different when compared to a resection margin of 4 cm (0.9 and 2.6%, respectively). A trend toward improved overall survival at 10 years was seen in the 4-cm group, 70 versus 77%, but this was not statistically significant.15
In the second Swedish Melanoma Study Group Trial, 936 patients with a melanoma greater than 2-mm thick were randomized to margins of either 2 cm or 4 cm. The authors reported no statistically significant differences in local recurrence or overall survival between the two arms.16
Haigh et al conducted a meta-analysis and systematic review of three of these trials (WHO, Intergroup Trial, and the first Swedish Melanoma Study Group Trial). When the data were combined, local recurrence, disease-free survival, and mortality were not statistically different between patients with primary cutaneous melanoma up to 4 mm in thickness undergoing excision with 1 cm to 2 cm margins compared to those randomized to 3 cm to 5 cm margins.17
Taken together, the data from all of these studies support the recommendation of 1 cm margins for a thin melanoma and 1 cm to 2 cm margins for an intermediate thickness melanoma. Although no randomized trials have directly compared 1 cm versus 2 cm margins for an intermediate thickness melanoma, we use a 2 cm margin for most melanomas that are 2 mm in thickness or greater except in anatomically constrained areas like the face, ears or distal extremities, where only a 1 cm margin can routinely be obtained. For a melanoma between 1.1 mm and 2 mm in thickness, a 1 cm margin is acceptable when the narrower margin allows for primary closure but a 2 cm margin would require skin grafting or significant tissue undermining to achieve closure. We are particularly likely to use a 1 cm margin for melanomas in this thickness range that are nonulcerated, with a relatively low mitotic rate and no evidence of angiolymphatic invasion. We have shown that using a 1 cm margin in this setting was associated with an acceptably low rate of local recurrence.18
4.3.3 Thick Melanoma
The NCCN recommends that thick melanomas, defined as tumors greater than 4 in thickness, should be resected with a 2 cm margin.12 A large, multi-institution retrospective (non-randomized) study of over 270 patients reviewed outcomes in patients with a thick melanoma who had a resection margin of either 2 cm or greater than 2 cm. Margins wider than 2 cm did not improve outcomes, given that local recurrence, disease-free survival, and overall survival were not significantly different between the two treatment arms after a median follow-up of 27 months.19
Thomas et al randomized 900 patients with tumor thickness of 2 mm or greater to excision with either a 1 cm or 3 cm margin. After a median follow-up of 60 months, there was increased locoregional recurrence in the 1 cm arm (p = 0.05), but no significant difference in overall survival between the arms. This study prohibited any form of nodal staging, be it elective lymph node dissection or sentinel lymph node biopsy. The absence of nodal evaluation raises an important point when considering the impact of the results of this trial. If lymph node evaluation had been conducted, there is a possibility that there would have been an imbalance in regional nodal disease between the two arms, which may have attributed more to the locoregional recurrence rate than the actual margin of excision. When only local and in-transit recurrences were considered, there were 37 recurrences in the 453 patients on the 1-cm arm (8.2%) versus 25 in the 447 patients on the 3-cm arm (5.6%), a difference that was not statistically significant. But there were 20 more nodal basin recurrences in the 1 cm arm than in the 3-cm arm, reinforcing the possibility that any observed outcome differences were at least partially related to imbalances in the number of stage III patients in each arm rather than an effect of the surgical treatment.20 While there are no data directly comparing a 2 cm and a 3 cm margin for thick melanoma, whenever a 2 cm margin has been prospectively or retrospectively compared to a wider (4 cm or 5 cm) margin, there has been no evidence of an advantage for the wider margin. Hence, we do not recommend either a 1 cm or a 3 cm margin for a thick melanoma, but rather routinely use a 2 cm margin whenever anatomically feasible, even if it requires a reconstruction to achieve this margin.
4.4 Sentinel Lymph Node Biopsy
While the margin of resection is important for control of local disease, melanoma frequently metastasizes via the lymphatic system, and the regional nodal basins are the most common site of melanoma metastasis. Evaluation of the nodal basin may be indicated at the time of initial wide excision. The sentinel lymph node represents the first lymph node in the lymph node basin directly draining the primary tumor. If the melanoma has metastasized via lymphatic channels, the sentinel lymph node would be the first lymph node to contain tumor deposits. The status of the regional nodes as determined by sentinel lymph node biopsy to determine the presence or absence of metastatic disease has been shown in a prospective randomized trial to be the most important prognostic factor in patients with clinically localized, intermediate-thickness melanoma.21
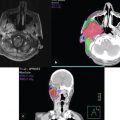
Sentinel lymph node biopsy should be performed in appropriately selected patients with clinically negative regional nodes at the time of wide excision of the primary tumor. A dual localization technique utilizing both injection of radiocolloid and injection of vital blue dye, either isosulfan blue or methylene blue, is most commonly used. The blue dye allows for direct visualization of the lymphatic channel and the sentinel lymph node itself. The use of blue dye alone has allowed the sentinel node to be identified in approximately 85 to 90% of cases, but the combination of both radiocolloid and blue dye increases the success rate to over 99%.22 We utilize isosulfan blue whenever a vital blue dye is employed, and do not use methylene blue for sentinel node localization at all due to higher reported local complication rates.23 One-half to 1 mCi of radiocolloid labeled with 99mtechnetium is injected intradermally, generally 1 to 4 hours before surgery, but if necessary the injection may be performed up to 24 hours prior to surgery.22 A variety of different radiocolloids are used around the world (e.g., sulfur colloid, tilmanocept, albumin nanocolloid and antimony trisulfide), with little or nothing in the way of head-to-head comparison data to determine which might be superior.24,25 Whichever and whenever the radiocolloid is injected, planar or computed tomographic lymphoscintigraphy is performed during the hour immediately thereafter in order to delineate the number and general location of the sentinel nodes. After the induction of anesthesia in the operating room, the vital blue dye is injected intradermally around the biopsy site or the primary tumor. A total volume of 0.5 to 1.5 mL is generally sufficient to identify the sentinel lymph nodes. Intraoperatively, a handheld gamma probe helps to direct the trajectory of dissection and guide the surgeon down to the “hot” and usually blue sentinel node(s).
Despite the high rate of accuracy with a dual localization technique, some surgeons do not routinely use blue dye. The choice to use radiocolloid alone may be due to limited availability of vital blue dye, concern that the use of blue dye will stimulate an allergic reaction, or because the patient is pregnant (we do not use blue dye during pregnancy because a maternal allergic reaction could be catastrophic for the fetus).23,26,27,28,29 In the Multicenter Selective Lymphadenectomy Trial-I (MSLT-1), the incidence of allergic reaction after isosulfan dye injection was only 0.2%,30 and in our experience the incidence of allergic reactions is even lower than that. Hence, we routinely utilize isosulfan blue dye in nonpregnant patients. One other issue relating to the use of vital blue dye is the presence of a tattoo on the skin in the drainage area of the nodal basin(s) undergoing sentinel node biopsy. Tattoo ink gradually leaches out of the skin site and accumulates in the regional nodes, coloring them enough to be easily seen. If the tattoo contained blue, green, or black ink, pigments within the node can be confused with vital blue dye or even metastatic melanoma.31 For this reason, we sometimes do not use vital blue dye in cases where a large tattoo is in the same draining basin as the primary melanoma, and focus our attention only on the radioactivity within the nodes.
The morbidity associated with sentinel lymph node biopsy is low, but potential complications include seroma, lymphocele, wound infection, and, in very rare cases, lymphedema.30,32 The morbidity of sentinel lymph node biopsy has been evaluated in prospective clinical trials. In MSLT-1, the rate of complications for patients undergoing sentinel lymph node biopsy was 10.1%.30
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


