9 Common Reconstructive Techniques after Facial Skin Cancer Excision Skin cancer represents a diverse collection of pathology. Skin cancer is the most common cancer in the United States, and it is estimated that 20% of Americans will develop at least one skin cancer in their lifetime.1,2 According to published figures, the average annual treatment cost for skin cancer in the United States was approximately $8.1 billion from 2007 to 2011.2 This figure continues to rise annually. A large subsection of skin cancer affects the face, given it is one of the areas that is most exposed to the elements. Cutaneous defects of the face are unique for a variety of reasons. From a medical science standpoint, wounds tend to heal very well with a low rate of infection and often require minimal debridement compared to other areas of the body due to the exceptional vascularity of the face. As will be discussed later, cosmetically acceptable results can be achieved even with secondary intention. From a social science standpoint, the face is critical for communication, as well as negotiating complex social interactions that are part of daily activity. Thus, reconstruction of lesions of the face is crucial for patients to maintain normalcy. Tagliacozzi—one of the fathers of plastic surgery—described it best, “restore, repair, and make whole those parts which nature has given, but fortunate has taken away, not so much that it please the eye of the beholder, but that it buoys the spirit of the afflicted.”3 Facial reconstruction allows for contributions from a range of specialties, including general and plastic surgery, dermatology, ophthalmology, and otolaryngology. In order to appropriately manage these defects, a multitude of options are necessary in the surgeon’s armamentarium. This requires exposure to extensive modalities from primary closure to skin grafting to locoregional flaps and even free tissue transfer. While some reconstructive options extend beyond the scope of this chapter, common techniques are described, including pitfalls to avoid. The face is one of the most anatomically complex aspects of the body. To aid surgeons in better elucidating areas of reconstruction, it has been divided into facial aesthetic regions based on landmarks and shadowing. The main aesthetic subunits of the face include the forehead, eyelids, cheeks, nose, lips, chin, and ears.4 These subunits are then subsequently further subdivided. For example, the nose itself has nine subunits: the dorsum, paired lateral side walls, tip, paired soft tissue triangles, paired lobules, and the columella.5 The ideal reconstruction for cutaneous defects provides coverage with like tissue, ideally from within the aesthetic unit itself. By manipulating the subunit principle, scars can be “hidden” within natural shadows to provide aesthetically pleasing outcomes for patients who present with initially intimidating facial defects. Experience in forehead reconstruction has revealed that large defects can be primarily closed with excellent results. Additionally, due to the rich vascularity, defects can also heal with secondary intention yielding cosmetically satisfying results ( Arterial and venous flow is provided by paired vessels. From the arterial standpoint, flow is distributed from both the external and internal carotid arteries by the paired frontal branches of the superficial temporal artery (external carotid artery system) and supratrochlear and supraorbital arteries (internal carotid artery system). Each supply is robust enough to allow for elevation of a flap utilizing this as the axial system. This allows for a variety of rotation and advancement flaps. The forehead is innervated by the supraorbital nerve as well as by the frontal branch of the facial nerve. The supraorbital nerve provides sensory innervation to the forehead and has two divisions. There is a deep division that runs from the orbital rim (lateral) toward the superior temporal line of the skull, which then moves cranial (parallel) to the temporal line before taking a medial course to enter the scalp. The superficial division also courses over the orbital rim, but traverses anterior to the frontalis muscle to provide sensation to the scalp. Injury to these nerves can lead to paresthesias as well as itching. The frontal branch of the facial nerve is deep to the frontalis—which it innervates. It provides motor function and can be identified along a line—referred to as Pitanguy’s line—that runs 0.5 cm below the tragus to a point 1.5 cm superior to the lateral position of the eyebrow.7 Small defects of the forehead—up to 1 to 2 cm—can be closed primarily or heal with secondary intention with satisfactory cosmetic results. This concept has been utilized in nasal reconstruction, where forehead flaps have been utilized for large nasal defects. The superior aspect of the forehead flap—which is based on an axial blood supply from the supratrochlear system—is left open to allow for granulation and healing. With standard wound care to ensure maintenance of a clean, moist environment, the forehead scarring is acceptable. The downside to leaving the wound open is that it may take up to 6 weeks to achieve complete healing. Medium-sized defects of the forehead—up to 3 to 4 cm—can be approximated with primary closure. Primary closure of larger wounds is possible in this region due to the excellent vascularity. Wounds that may otherwise develop wound necrosis elsewhere on the body due to tension on the incision often heal without complication. For relatively large defects of the forehead—up to 6 cm—advancement flaps provide excellent outcomes as they mobilize skin from relaxed skin tension lines (RSTL) of the forehead. While full-thickness, sheet skin grafts are also excellent options, “H-flaps” allow for reconstruction within the aesthetic principle without utilization of a separate donor site. H-flap also utilizes the benefit of increased laxity found within the lateral forehead skin, which helps to facilitate mobilization. In prospective case series studies, H-flap was found to have excellent cosmetic outcomes based on answers to a validated patient satisfaction questionnaire.8 The flap is created by making incisions parallel to the RSTL and removing burrow triangles from each side. After removal of the triangles and undermining superficial to the temporal muscle to decrease the likelihood of injury to the supraorbital nerves, the wounds can be closed without undue tension, also allowing for aesthetic scars ( Fig. 9.1 (a,b) Secondary healing of a forehead after a paramedian forehead flap utilized for nasal reconstruction is common practice. Often, acceptable cosmetic results can be obtained using this method for the forehead. (c) The superior aspect was left to heal with secondary intention leaving a cosmetically acceptable result. Temporal wounds of the forehead can also be reconstructed using local advancement flaps, as described earlier. A key aspect in this region is to maintain the position of the eyebrow as well as the temporal hairline. Regional flaps—including the cervico-facial flap, which will be discussed in detail later in this chapter—can provide one with the ability to solve both of these potential situations before they become an issue. The cheek possesses the largest facial aesthetic region and is intimately related to social interaction as it allows for the ability to capture emotion on a large scale, in conjunction with the other aspects of the face. It marries the superior and inferior face to act as one unit. Contour of the cheek is created by a synergy of fat distribution, underlying bony architecture, and the retaining ligaments of the face. Retaining ligaments of the cheek are critical for these subunits as they provide the structural framework that allows for youthful appearance. Thus, as one ages, these ligaments become increasingly lax, which can cause fat redistribution, leading to an older appearance. Several of these retaining ligaments have been described which has allowed for classification of the aforementioned creases. For example, the retaining ligaments of the zygoma have been referred to as McGregor’s patch. These are osteocutaneous ligaments that provide support for the skin overlying the zygoma. Other examples include ligaments at the junction of the cheek and upper lip creating the melolabial (nasolabial) crease.9 The anatomy of the cheek requires knowledge of the facial nerve as well because injury can be severely disfiguring for patients. As long as dissection proceeds anterior to the superficial musculoaponeurotic system (SMAS), a safe plane—with respect to the nerves—is maintained. Fig. 9.2 A 2-cm squamous cell carcinoma excised leaving a 6-cm defect approximated with an H-flap under local anesthesia. Fig. 9.3 An easy-to-follow cheek reconstruction algorithm. (Reproduced with permission from Rapstine et al.11) The cheek receives its vascular supply from the external carotid system. Namely, it obtains the majority of its blood flow from branches of the facial artery. A minor supply is provided by the transverse facial artery, which is a branch of the superficial temporal artery. The venous drainage follows the arterial system, as it does in the forehead. Innervation to the cheek is dependent on location. The medial aspect of the cheek from just lateral of the lateral limbus to the upper second premolar tooth is supplied by the infraorbital nerve (from the second division of the trigeminal cranial nerve). The nerve also provides sensation to the lower eyelid, upper lip, and nasal vestibule. The anterior branch of the great auricular nerve provides sensation for the lateral skin from the tragus to the lateral limbus. Several classification systems of the cheek have been developed that divide the cheek into separate aesthetic subunits. One utilizes eight separate aesthetic subunits. They are the inferior bony orbital rim, nasofacial sulcus, melolabial crease, labiomandibular crease, inferior border of the mandible, preauricular crease, and a line extending from the lateral canthus to the root of the helix.9 Roth et al divided the cheek into three overlapping aesthetic zones: zone 1 (suborbital), zone 2 (preauricular), and zone 3 (buccomandibular).10 Based on these zones, reconstructive algorithms for the cheek have been described. Small defects that abut the nose/lip or chin can be closed using crescentic advancement, bilobed/VY advancement, or nasolabial fold flaps. For patients who have large defects of the cheek—more than 3to4cm—several options for reconstruction are feasible. While tissue expansion is an appropriate option and can lead to excellent results, it requires several weeks to months of painful expansion as well as substantial disfigurement in the time frame until the expansion process has reached its completion. Additionally, custom-made expanders are often required for the cheek, which can cause an increase in cost. Full-thickness skin grafting, harvested from the pre/postauricular or supraclavicular sites, provides a reasonable reconstructive option for older patients who possess multiple comorbidities. Skin grafting is not the preferred option given that it can be difficult to obtain a good color match with the native face. Furthermore, contracture of the skin graft can also lead to suboptimal results. Originally described by Mustarde for lower lid reconstruction, cervicofacial advancement flaps provide the ability to cover a large surface defect of the skin with tissue that possesses an ideal color, texture, and contour match.12 Austen et al described 32 consecutive cervicofacial flaps that were performed without major complications and with satisfactory cosmetic results.13 Additionally, dissection can be carried inferiorly beneath the neck to the level of the deltopectoral groove to assist in the recruitment of additional tissue for tension-free repair. This is of importance for wounds that are large and also are near the medial canthus, where excess tension of the wound can lead to ectropion (
9.1 Introduction
9.2 Forehead
![]() Fig. 9.1). The forehead has been subdivided into para-median, lateral, and lateral temporal subunits, with the eyebrows providing a mobile subunit of their own.6
Fig. 9.1). The forehead has been subdivided into para-median, lateral, and lateral temporal subunits, with the eyebrows providing a mobile subunit of their own.6
![]() Fig. 9.2). The cosmesis can be improved further by designing the flap in such a way that the horizontal components are able to fit within the main transverse rhytids of the forehead that are created due to the natural movement of the frontalis muscle.
Fig. 9.2). The cosmesis can be improved further by designing the flap in such a way that the horizontal components are able to fit within the main transverse rhytids of the forehead that are created due to the natural movement of the frontalis muscle.

9.3 Cheeks

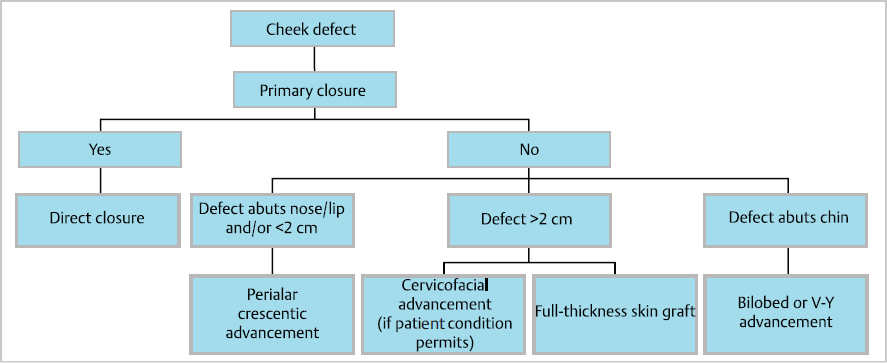
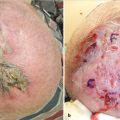
![]() Fig. 9.3 reveals an algorithm that is easy to follow in this author’s opinion.11 Many defects of the cheek—including a high percentage of Mohs defects—can be reconstructed using primary closure. An elliptical excision or simply creating Burow’s triangles at both ends of a Mohs defect, in the plane that is best fitting with the RSTL, allows for tension-free, primary closure with optimal cosmetic results. This is especially the situation in older patients because there is an increase in the amount of skin laxity, thus allowing for repair without concern for issues including ectropion or elevation of the modiolus.
Fig. 9.3 reveals an algorithm that is easy to follow in this author’s opinion.11 Many defects of the cheek—including a high percentage of Mohs defects—can be reconstructed using primary closure. An elliptical excision or simply creating Burow’s triangles at both ends of a Mohs defect, in the plane that is best fitting with the RSTL, allows for tension-free, primary closure with optimal cosmetic results. This is especially the situation in older patients because there is an increase in the amount of skin laxity, thus allowing for repair without concern for issues including ectropion or elevation of the modiolus.
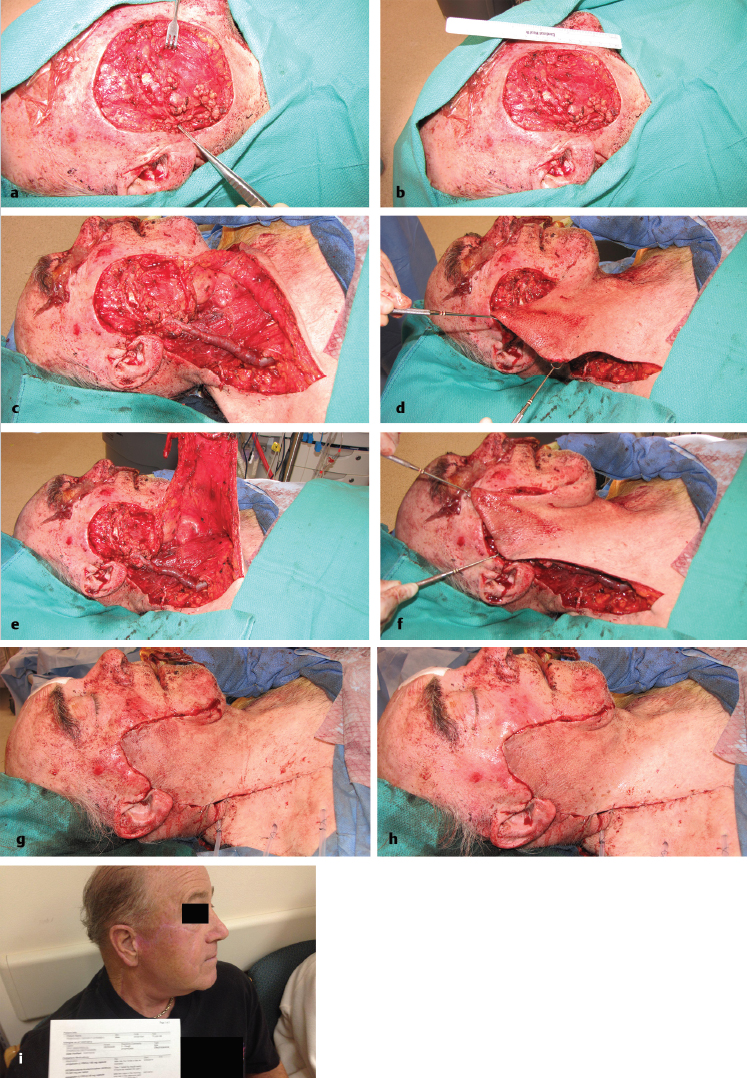
![]() Fig. 9.4). A significant aspect in the reconstructive decision tree is choosing between a cervicofacial and reverse cervicofacial advancement flap.14 The difference between the two types of flap stems from the directionality of the rotation. A cervicofacial flap rotates the lateral cheek and neck skin toward the nose. The reverse cervicofacial flap rotates the skin of the lower face in a cranial direction. The reverse flap is used in situations where the defect is medial to the midpupillary line (
Fig. 9.4). A significant aspect in the reconstructive decision tree is choosing between a cervicofacial and reverse cervicofacial advancement flap.14 The difference between the two types of flap stems from the directionality of the rotation. A cervicofacial flap rotates the lateral cheek and neck skin toward the nose. The reverse cervicofacial flap rotates the skin of the lower face in a cranial direction. The reverse flap is used in situations where the defect is medial to the midpupillary line (![]() Fig. 9.5).
Fig. 9.5).
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine