8 Surgical Implications of Systemic Therapy for Skin Cancer Skin cancer is the most common form of cancer worldwide. Basal cell and squamous cell carcinomas represent the vast majority of these cancers and are associated with sun and ultraviolet radiation exposure. In the United States, it is estimated that 3.5 million nonmelanoma skin cancers are diagnosed annually, with 20% being squamous cell carcinoma.1 While melanoma is far less frequent with 87,110 new cases expected in 2017, it accounts for at least 50% of mortality from all skin cancers. The incidence of melanoma has been steadily increasing by approximately 2.6% annually since the 1970s.2 Skin cancer mortality has also been increasing, largely related to the recent increase in squamous cell carcinoma deaths. In 2017, it is expected there will be almost 9,730 deaths from melanoma and up to 8,800 deaths from squamous cell carcinoma.2,3 While the prognosis for most patients diagnosed with skin cancer is excellent, major challenges exist in treating advanced squamous cell carcinoma and metastatic melanoma. Approximately 5% of all patients with squamous cell carcinoma (nearly 30,000 patients annually) have high-risk tumors with significant rates of regional and distant metastases.4 Most of the 8,791 deaths attributable to squamous cell carcinoma occur in these patients. Similarly, while 5-year survival rates for early-stage melanoma approach 98%, the overall survival for stage IV disease remains less than 20%.5 In the past few years, however, major advances in the treatment of patients with metastatic melanoma have occurred. The developments in targeted therapeutics and tumor immunotherapy have revolutionized the management of metastatic melanoma. From 2011 to 2015, there have been seven new U.S. Food and Drug Administration (FDA)-approved agents. The roles of targeted therapy and immunotherapy are also being explored in nonmelanoma skin cancers. During the 20th century and the first decade of the 21st century, only two agents were available for the treatment of meta-static melanoma. These were dacarbazine, an alkylating agent, and high-dose interleukin-2 (IL-2), an immunotherapy drug.6 Since 2011, multiple agents have been shown to improve progression-free and/or overall survival for patients with advanced melanoma. These include ipilimumab (a first-generation T-cell checkpoint inhibitor), vemurafenib and dabarafenib (BRAF inhibitors), and trametinib (a selective MEK inhibitor).7,8,9 Additionally, dramatic results with newer immunotherapy drugs, such as programmed death-1 (PD-1) and PD-1 ligand 1 (PD-L1) inhibitors, have been promising with two PD-1 inhibitors, pembrolizumab and nivolumab, being approved in 2014 for second-line treatment of metastatic melanoma. Several clinical trials are also under way to evaluate these new agents in the adjuvant treatment of melanoma and for the treatment of metastatic skin cancers, including squamous cell carcinoma and Merkel cell carcinoma. As the list of these agents grows and therapeutic efficacy improves, the number of people who are living longer with advanced melanoma is likely to rise. In these patients, the role of surgery in the treatment of metastatic disease will probably expand in order to augment the benefits of newer, more potent systemic therapies. Similarly, the surgeon must be familiar with the indications and toxicity profiles of these agents to maximize the benefit of surgical intervention in this new era of systemic cancer therapy. This chapter will briefly discuss the new systemic agents and highlight implications for surgical management, focusing on melanoma and squamous cell carcinoma. Treatment options for patients with metastatic melanoma include cytotoxic chemotherapy, targeted therapy, and immunotherapy. Surgical resection and radiotherapy are supplementary or palliative, and can be beneficial in carefully selected patients with minimal metastatic disease or isolated residual disease after systemic therapy. Consensus guidelines from the Society for Immunotherapy of Cancer (SITC) and the National Comprehensive Cancer Network (NCCN) are available to help choose the type and order of therapy for patients with advanced melanoma10,11 (http://www.nccn.org/professionals/physician_gls/PDF/melanoma.pdf). A multidisciplinary team consisting of medical, surgical radiation oncology, and molecular pathology and radiology is pivotal in providing appropriate treatment of such patients. Patients with advanced melanoma should be evaluated with a serum lactate dehydrogenase level, for the purposes of staging and monitoring response to treatment as well as whole-body imaging, with particular attention to visceral organs, central nervous system (CNS), and bone. For patients with disease that can be completely resected with negative margins, metastasectomy is indicated and has been associated with 30 to 35% 5-year survival.10,11 Radiation therapy has also been useful in patients with large, matted lymph node disease, especially in the neck and axillary nodal basins. It has also been beneficial in patients with painful bone lesions and CNS disease. While cytotoxic chemotherapy is not as effective for melanoma as for other cancers, it may still play a role in the management of the disease. The only chemotherapy agent approved by the FDA for the treatment of metastatic melanoma is dacarbazine (DTIC). It has been available since 1974.12 Less than 5% of patients experience a complete response, and 5-year survival rates range from 2 to 6%. However, objective response rates can be as high as 20%, and it is relatively well tolerated.13 DTIC remains the single-agent chemotherapy drug of choice given that no high-quality trial has shown a survival benefit with another chemotherapy drug. Temozolomide is an oral analog of dacarbazine with the added advantage of CNS penetrance. In a study that compared the two agents, there was no difference in objective response rate (21% with temozolomide vs. 18% with dacarbazine), overall survival (7.7 vs. 6.4 months; p = 0.20), or side effect profile.14 Temozolomide can be used in place of dacarbazine in the setting of brain metastases or if oral administration is desired. Multiple combination chemotherapy regimens have been studied in attempts to improve on the minimal efficacy of the above-described monotherapy. A combination of cisplatinum, vinblastine, and dacarbazine (CVD) has been widely used, but it has yielded increased toxicity without a survival benefit.15,16 A combination of carboplatin and paclitaxel in the setting of progression on dacarbazine or temozolomide has shown promising results in a phase II clinical trial.17 An objective response rate of 26% and an overall survival of 7.8 months were reported. Biochemotherapy, in which interferon alfa-2b (IFNα2β) and low-dose IL-2 are added to CVD, has also been tested in attempts to improve outcomes. However, two large randomized clinical trials have demonstrated an increase in adverse events without improvement in overall survival when compared to standard chemotherapy.18,19 Multiple molecular pathways with gene mutations that drive tumor progression in melanoma cells have been identified, resulting in the development of molecular inhibitors. BRAF inhibitors, MEK inhibitors, vascular endothelial growth factor (VEGF) inhibitors, and CKIT inhibitors are all pertinent to the discussion of targeted therapy in melanoma. The BRAF pathway utilizes RAS-RAF-MEK-ERK signaling proteins ( The first BRAF inhibitor, vemurafenib, was approved by the FDA in 2011 for use in BRAF-mutated metastatic melanoma.8 In a phase III clinical trial of 675 treatment-naive patients, vemurafenib was compared to dacarbazine, and was associated with an improvement in progression-free survival (5.3 vs. 1.6 months, p < 0.001) and 6-month survival (84 vs. 64%). Tumor regression was seen in up to 50 to 70% of patients across clinical trials.8,21,22 Median time to response was short—approximately 4.5 weeks; however, resistance was common, typically within 7 to 8 months after the initiation of therapy. Several strategies, such as combination therapy and discontinuous dosing, are being attempted in order to lower the emergence of resistance. Dabrafenib is another BRAF inhibitor that has also demonstrated improved progression-free survival compared to dacarbazine (5.1 vs. 2.7 months, p < 0.001), with an objective response rate of 52%.23 As a result of this trial, dabrafenib was approved by the FDA in 2013. Both vemurafenib and dabrafenib can be taken orally. Both have a slightly higher toxicity profile than dacarbazine, and dose reduction may be necessary in up to 38% of patients.8 The adverse events of these agents include fatigue, arthralgias, myalgias, skin hypersensitivity, and development of skin lesions, such as acanthomas and cutaneous squamous cell carcinoma. Trametinib, an oral MEK inhibitor that has been FDA-approved since 2013, was tested against dacarbazine or paclitaxel in a phase III clinical trial that included 322 patients with BRAF V600E or V600K mutation metastatic melanoma.24 Progression-free survival (4.8 vs. 1.5 months, p < 0.001) and 6-month survival (81 vs. 67%, p = 0.01) were both superior with trametinib. Objective response rate was 22%, which was lower than with BRAF inhibitors, and reported side effects were fewer. Skin reactions were common, such as rash, dermatitis, acneiform, dry skin, pruritus, and paronychia. However, these were generally mild. Other side effects included diarrhea, stomatitis, abdominal pain, lymphedema, hypertension, and hemorrhage. Fig. 8.1 BRAF pathway and cell signaling. Mutations in MEK may be responsible for resistance to BRAF inhibitors. A phase II clinical trial was conducted in which 162 patients were treated with either dabrafenib alone or a combination of dabrafenib and trametinib.9 Median progression-free survival was considerably improved with dual therapy from 5.6 to 9.4 months, while the objective response rate was 76 versus 54% (p = 0.03). Interestingly, the development of squamous cell carcinoma, which is seen in about 20% of patients with mono-therapy BRAF inhibitors, was more than halved by the addition of the MEK inhibitor. Depending on the dose of trametinib, the incidence of squamous cell carcinoma ranged from 2 to 7% (p = 0.004 and 0.09). While other skin changes associated with BRAF inhibitors were less frequent in the combination therapy group, MEK inhibitor–associated toxicities were common. More recently, these findings were replicated in the setting of a phase III clinical trial that included 423 previously untreated patients.25 In the dual therapy group, there was an improvement in progression-free survival (9.3 vs. 8.8 months, p = 0.03), objective response rate (67 vs. 51%, p = 0.002), and 6-month survival (93 vs. 85%, p = 0.02). Similarly, the incidence of squamous cell carcinoma was lower in the combination therapy group (2 vs. 9%). VEGF and CKIT represent other possible therapeutic targets for drug development in melanoma. There has been lack of efficacy with anti-VEGF agents when used alone, and somewhat disappointing results when used in combination with cytotoxic chemotherapy.26 In the setting of a phase II clinical trial, 214 patients were treated with carboplatin and paclitaxel with or without bevacizumab. The differences in progression-free survival (5.6 vs. 4.2 months), objective response rate (25.5 vs. 16.4%), and median overall survival (12.3 vs. 9.2 months) all failed to reach statistical significance. Imatinib, a CKIT inhibitor, has significantly improved outcomes in patients with gastrointestinal stromal tumors and chronic myelogenous leukemia. CKIT mutations are present in approximately 6% of all melanomas, but higher rates have been reported in patients with mucosal and subungual lesions.27 A phase II clinical trial was conducted in which 24 patients with CKIT-mutated melanoma were treated with imatinib, and an objective response rate of 29% was reported.28 The disease control rate was 50%, but varied considerably between CKIT mutations and CKIT amplifications (77 vs. 18%).28 These data suggest there may be a role for VEGF and CKIT inhibition, but to date, the results of clinical trials have not been sufficient to mandate clinical approval of these agents. Nonetheless, melanoma patients may be exposed to these drugs as part of clinical trials. Immunotherapy can be defined as the augmentation of the host immune system to combat cancer cells. This is possible because B and T cells can recognize tumor-associated antigens, resulting in cytotoxicity of tumor cells. This process can initiate a cascade of immune responses against multiple antigens released by dying tumor cells leading to the eventual elimination of tumor. The important role of T cell–mediated immunity has been widely recognized, leading to the development of several immunotherapy agents designed to promote activation or prevent inhibition of T cell responses. These include cytokines, such as interferon and IL-2, and, more recently, inhibitors of T cell checkpoints, such as ipilimumab, pembrolizumab, and nivolumab. All five aforementioned agents, as well as a pegylated form of interferon, have been approved by the FDA for the treatment of metastatic melanoma. In contrast to chemotherapy and targeted therapy, which are associated with rapid onset of response with eventual resistance, immunotherapy may have a more delayed onset of activity without the association with resistance. It often can also induce durable responses, even in patients with advanced metastatic disease. IL-2, which was approved by the FDA for metastatic melanoma treatment in 1998, had been extensively studied for three decades in mouse models as well as human clinical trials. The exact antitumor mechanism is unclear, but IL-2 appears to function by promoting large volume expansion of tumor-specific effector T cells. Two large trials were integral in testing the effectiveness of IL-2. A single-institution clinical trial, which included 409 patients with either metastatic melanoma (n = 182) or renal cell carcinoma (n = 227), demonstrated that high-dose IL-2 led to an objective response rate of 17.1%, with 8.1% of patients achieving a complete response.29 A subsequent multi-institutional clinical trial in 270 patients with metastatic melanoma showed similar results, with an objective response rate of 16% and a complete response rate of 6%.30 Perhaps, the most remarkable finding of the trial was the durability of the responses. In the responder group, the median duration of complete response was 59 months, and 40% of patients were disease-free for over 70 months.31 Therapy with IL-2 is associated with considerable morbidity related to capillary leak syndrome. However, toxicities are usually reversible and guidelines exist to help clinicians manage these.32 Ipilimumab is a monoclonal antibody that targets the T cell checkpoint inhibitor, cytotoxic T-lymphocyte antigen-4 (CTLA-4), found on the surface of activated T cells ( Fig. 8.2 Various T-cell pathways and sites of action of immunotherapy agents in melanoma. Ipilimumab has also been used in combination with dacarbazine or granulocyte-macrophage colony-stimulating factor (GM-CSF) in two large clinical trials.33,34 When used in conjunction with dacarbazine, 1-year survival was significantly improved (47.3 vs. 36.3%).33 However, grade 3 or higher adverse events were more than doubled in the combination group (56.3 vs. 27.5%, p < 0.001). When given together with GM-CSF, 1-year survival was significantly improved over ipilimumab alone (68.9 vs. 52.9%, p = 0.01), but the combination was paradoxically associated with fewer side effects.34 Adverse events associated with ipilimumab include autoimmune dermatitis, colitis, hepatitis, hypophysitis, and rarely peripheral neuritis and pancreatitis. Early detection is paramount to treatment, as therapy discontinuation, administration of corticosteroids, and, in rare cases, infliximab have been shown to be successful in the management of the autoimmune-related toxicities.35 The PD-1 receptor is another T cell checkpoint that is expressed on the surface of T cells after activation ( In a phase I clinical trial, 135 melanoma patients were treated with an anti-PD-1 antibody in a dose escalation manner.37
8.1 Introduction
8.2 Systemic Therapy of Melanoma
8.2.1 Chemotherapy
8.2.2 Targeted Therapy
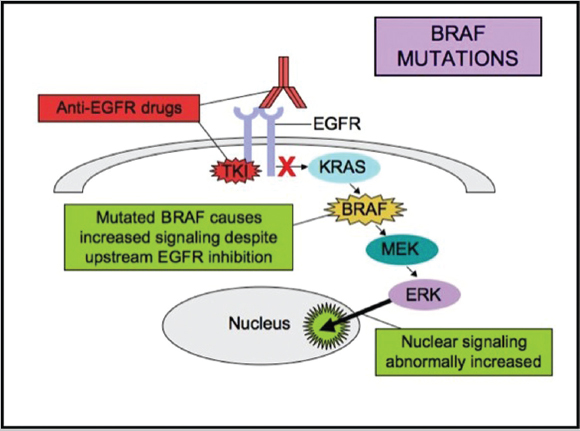
BRAF and MEK Inhibitors
![]() Fig. 8.1). BRAF mutations lead to constitutive activation of the pathway and are critical to cell signaling, tumor growth. Activating mutations in BRAF occur in approximately 50% of cutaneous melanomas.20 Mutations in RAS, BRAF, and MEK proteins lead to continuous activation of the pathway despite the absence of a growth ligand. The most common BRAF mutation is at amino acid position 600 resulting in an exchange of valine for glutamic acid (V600E). All patients with advanced melanoma should be tested for BRAF mutation because of its relatively high prevalence and potential pharmacologic treatment options.
Fig. 8.1). BRAF mutations lead to constitutive activation of the pathway and are critical to cell signaling, tumor growth. Activating mutations in BRAF occur in approximately 50% of cutaneous melanomas.20 Mutations in RAS, BRAF, and MEK proteins lead to continuous activation of the pathway despite the absence of a growth ligand. The most common BRAF mutation is at amino acid position 600 resulting in an exchange of valine for glutamic acid (V600E). All patients with advanced melanoma should be tested for BRAF mutation because of its relatively high prevalence and potential pharmacologic treatment options.
Anti-VEGF and CKIT Inhibitors
8.2.3 Immunotherapy
Interleukin-2
Ipilimumab
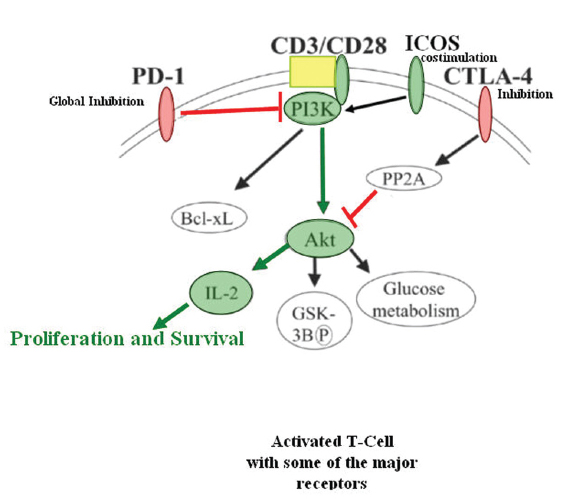
![]() Fig. 8.2). T cells are activated through a series of signals, with the first signal provided by the T cell receptor upon recognition of cognate antigen presented as processed peptides bound to major histocompatibility complexes. The second signal is provided by CD28, which is also found on the surface of T cells, activating proliferation and cytokine production upon binding to the costimulatory molecules, B7.1 and B7.2. After activation, CTLA-4 is mobilized to the T cell surface and modulates T cell activity by binding B7.1 and B7.2 with high affinity and inhibiting T cell proliferation and cytokine production. Ipilimumab prevents CTLA-4 from inhibiting T cell activity and hence prevents T cell inhibition, allowing a more prolonged, and thus potent, T cell response. In a phase III clinical trial of 676 patients with advanced melanoma, patients were randomized to ipilimumab alone, combination with a gp100 peptide vaccine, or both. There was an improvement in overall survival with ipilimumab (10 vs. 6 months, p = 0.0026) given alone or in combination compared to vaccine alone.7 Interestingly, there was no significant difference in progression-free survival between treatment arms, suggesting a delayed therapeutic response with ipilimumab.
Fig. 8.2). T cells are activated through a series of signals, with the first signal provided by the T cell receptor upon recognition of cognate antigen presented as processed peptides bound to major histocompatibility complexes. The second signal is provided by CD28, which is also found on the surface of T cells, activating proliferation and cytokine production upon binding to the costimulatory molecules, B7.1 and B7.2. After activation, CTLA-4 is mobilized to the T cell surface and modulates T cell activity by binding B7.1 and B7.2 with high affinity and inhibiting T cell proliferation and cytokine production. Ipilimumab prevents CTLA-4 from inhibiting T cell activity and hence prevents T cell inhibition, allowing a more prolonged, and thus potent, T cell response. In a phase III clinical trial of 676 patients with advanced melanoma, patients were randomized to ipilimumab alone, combination with a gp100 peptide vaccine, or both. There was an improvement in overall survival with ipilimumab (10 vs. 6 months, p = 0.0026) given alone or in combination compared to vaccine alone.7 Interestingly, there was no significant difference in progression-free survival between treatment arms, suggesting a delayed therapeutic response with ipilimumab.
PD-1 and PD-L1 Inhibitors
![]() Fig. 8.2). Although PD-1 expression is observed shortly after T cell activation, it serves as a marker of T cell exhaustion and functions similarly to CTLA-4 in downregulating T cell responses. PD-1 signaling is triggered by binding to one of two ligands, called PD-L1 and PD-L2.36 Inhibition of PD-1 binding to PD-L1 has been proposed as another strategy for preventing or reversing T cell exhaustion, and this has shown significant promise in the treatment of melanoma, non–small cell lung cancer, bladder cancer, Hodgkin’s lymphoma, and other cancers. In 2014, two PD-1 inhibitors, pembrolizumab and nivolumab, were FDA-approved for the treatment of metastatic melanoma in the second-line setting.
Fig. 8.2). Although PD-1 expression is observed shortly after T cell activation, it serves as a marker of T cell exhaustion and functions similarly to CTLA-4 in downregulating T cell responses. PD-1 signaling is triggered by binding to one of two ligands, called PD-L1 and PD-L2.36 Inhibition of PD-1 binding to PD-L1 has been proposed as another strategy for preventing or reversing T cell exhaustion, and this has shown significant promise in the treatment of melanoma, non–small cell lung cancer, bladder cancer, Hodgkin’s lymphoma, and other cancers. In 2014, two PD-1 inhibitors, pembrolizumab and nivolumab, were FDA-approved for the treatment of metastatic melanoma in the second-line setting.
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


