Chapter 46 Treatment of liposuction complications
• Correction after the occurrence of a complication in lipoplasty is very difficult, hence prevention of complications is crucial.
• Surgical tips for preventing complications are given (see video clip 1).
• Maintainance of the multiple spheres and angles of the body rather than converting the region into a single plane is important.
• Perform circumferential liposuction using a smaller diameter cannula.
• Superficial suction leads to dimple depression (“contour irregularities”). Deep suction leads to adhesions.
• Perform serial liposuction procedures rather than large volume liposuction.
• Prevent lethal complications, using the time gap protocol.
Introduction
Numerous cannulae and instruments have been introduced for use in liposuction.1–3 The tumescent technique and the concept of ultrasonic or laser lipolysis are now widely accepted to assist in more advanced and safe liposuction procedures.4 Even with the considerable advancements in techniques aided by various new instruments, the complications related to liposuction, however minor, are still a concern.5 Moreover, numerous previous studies in the literature have focused on and highlighted safety considerations in liposuction. There is a lack of strategy and treatment guidelines for complications of liposuction. In this chapter, a good guideline for the treatment of complications from liposuction is provided, which range from life-threatening to esthetic complications.
Complications and Their Management
Life-threatening or Systemic Complications
Fat Embolism Syndrome (FES)
Diagnosis using ventilation–perfusion scan may show the matching defects.6–8 Differential diagnoses include fluid overload, pulmonary edema, aspiration pneumonia and various other causes of acute respiratory distress syndrome (ARDS).9 Most of all, differentiation of FES from pulmonary embolism is important because the treatment is very different. Heparin can be harmful, for obvious reasons, in the early management of FES.
Treatments using intravenous ethanol, heparin, and low molecular weight dextran have largely fallen from favor. Medical management now consists mainly of high-dose corticosteroids, which have been shown to prevent the development of FES in several prospective randomized trials.10–12 The role of corticosteroids is considered to inhibit the inflammatory reaction to the presence of fat in the circulatory system after liposuction.
Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)
There are three major factors that are important in the development of DVT and PE. The first is the development of venous stasis, the second is the activation of a blood coagulation cascade, and the third is injury to the vascular endothelium (Virchow’s triad).13
Initial therapy consists of intravenous heparin, usually by a bolus dose of 5000 to 10 000 U.
Extended Infection
Liposuction involves heavy manipulation of the superficial fascial system, resulting in the possibility of ascending infections via the fascial system, and there have been reports of necrotizing fasciitis from these procedures.14 Although infection in simple liposuction cases is rare, combined procedures including abdominoplasty and brachioplasty for reduced skin laxity may cause serious infections. Hematomas and seromas can become sources of infection, hence meticulous hemostasis and drainage of seromas is important to prevent infection (Figs 46.1 and 46.2). Moreover, maintaining aseptic techniques throughout the procedure is of utmost importance, especially during positional changes of the patient.


FIG. 46.2 Severe wound infection on right posterior thigh with a draining sinus.
(From Kim YH, et al. Analysis of postoperative complications for superficial liposuction: A review of 2398 cases. Plast Reconstr Surg 2011;127:863–871. with permission.)
Hypovolemia/Anemia
Tumescent infiltration provides profound hemostasis in large volume liposuction.15 Bloodless aspiration virtually eliminates the possible sequelae of shock and hypovolemia. The ideal ratio of subcutaneous fluid to total aspirate is controversial. The surgeon must weigh the risks between excessive blood loss (inadequate subcutaneous fluid) and pulmonary edema (excess subcutaneous fluid). Fluid shifts between interstitial fluid and plasma volume can result in intravasation (hypervolemia) or extravasation (third spacing). Excessive infiltration obviously should be avoided. According to our 14-year experience with 2398 cases, the need for blood transfusions is rare. It must be remembered that 2000 ml aspiration of supernatant fat is regarded as a decrease in hemoglobin count by 1. Some of the drawbacks of blood transfusions include potential infection, transfusion mismatch, circulatory overload, microthrombi, and postoperative anemia.
Healthy normovolemic patients can tolerate a moderate reduction in hemoglobin count with multiple compensatory mechanisms. In clinical settings, normal tissue oxygenation is maintained with hematocrits as low as 20, if the subject is healthy and remains normovolemic.16
Lidocaine Toxicity
Early signs and symptoms of lidocaine toxicity include lightheadedness, restlessness, drowsiness, tinnitus, slurred speech, metallic taste in the mouth, and numbness of the lips and tongue. These subjective signs may be seen at plasma levels between 3 and 6 µg/ml. Shivering, muscle twitching, and tremors may occur as plasma levels reach 5–9 µg/ml, followed by convulsions, CNS depression, and then coma at plasma levels greater than 10 µg/ml. As levels increase above this, respiratory depression and eventually cardiac arrest can occur.17
Esthetic Complications
Contour Irregularities (Figs 46.3–46.7)


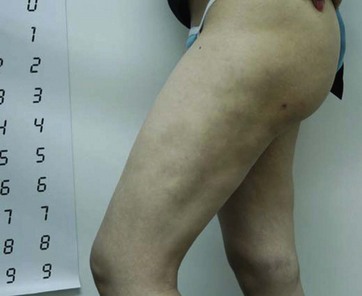
FIG. 46.5 Contour irregularities on lateral aspect of thigh with induction of fibrous and dense tissues.

FIG. 46.6 Severe contour irregularity at the trunk and thigh regions.
(From Kim YH, et al. Analysis of postoperative complications for superficial liposuction: A review of 2398 cases. Plast Reconstr Surg 2011;127:863–871. with permission.)
Related posts:
 Brachioplasty with liposuction resection
Brachioplasty with liposuction resection
 Liposuction of the abdomen and trunk
Liposuction of the abdomen and trunk
 Short vertical scar medial thigh lift
Short vertical scar medial thigh lift
 Upper body lift with lateral excision
Upper body lift with lateral excision
 Autologous gluteal augmentation with mid-pedicle superior pole perforator flaps
Autologous gluteal augmentation with mid-pedicle superior pole perforator flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


