| Primary canaliculitis resistant to medical management (digital massage, warm compresses, targeted topical or oral antimicrobials, and repeated irrigation) |
| Secondary canaliculitis resistant to plug removal and irrigation |
| Punctal stenosis or canalicular obstruction associated with canaliculitis |
| Recurrent primary or secondary canaliculitis |
| History of prior intracanalicular plug (SmartPlug, hydrogel, silicone, or collagen) |
| History of prior head and neck malignancy (squamous cell carcinoma, inverting papilloma, etc.) |
| Check for patency of the lacrimal drainage system by irrigation |
Introduction
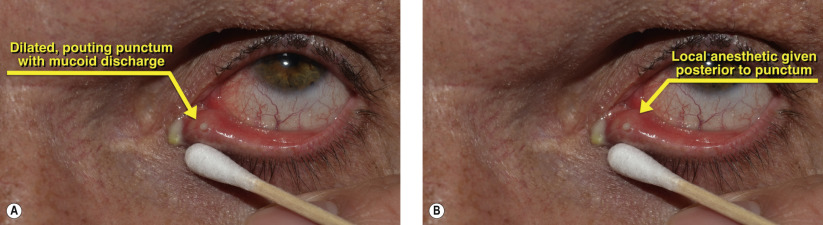
Canaliculitis is an infection of the canaliculus and the proximal lacrimal ducts. It classically presents with epiphora, medial eyelid swelling, conjunctivitis, and a characteristically elevated pouted punctum with mucopurulent discharge ( Figure 61.1A ). Canaliculitis is often confused with chalazia but is distinguished by its centration about the punctum where the meibomian glands are not present.
Classically, concretions or sulfur granules are expressed from the punctum by retrograde massage and are associated with infection by Actinomyces spp., a filamentous Gram-positive rod . Infection or co-infection with Streptococcus and Staphylococcus are also seen.
Canaliculitis can be primary or secondary to instrumentation such as lacrimal intubation or plug insertion. Intracanalicular occlusion by the SmartPlug and Herrick plug has been associated with secondary canaliculitis. These intracanalicular devices cause tear stasis and act as a nidus for infection and can be posteriorly dislodged further down the lacrimal system by irrigation. With more distal obstruction and scarring, an open surgical approach is often necessary for removal. Permanent scarring of the common canaliculus may necessitate conjunctivodacryocystorhinostomy ( Chapter 59 ).
Primary canaliculitis is treated conservatively with warm compresses, retrograde digital massage, along with topical and oral antibiotics. Repeated irrigation of the lacrimal system with antibiotics has also been advocated as an alternative to surgical treatment.
Once the canaliculus becomes impacted by progressively larger concretions, medical management gives way to definitive surgical intervention. The procedure begins with a canaliculotomy to expand the posterior aspect of the punctal ring and then meticulous expression and curettage of impacted concretions. Antibiotic irrigation of the lacrimal system can also be performed as an adjunctive procedure. Recurrent canaliculitis warrants histopathology and cultures to rule out neoplasm and resistant organisms.
Surgical Technique