The aim of reconstructive nasal surgery is not only to rebuild all or part of the nose but also to blend and tailor the new and old tissues in such a way as to create the best possible result. Although a variety of reconstructive options exist, local or regional skin flaps are one of the most powerful reconstructive tools for the reconstruction of cutaneous nasal defects. This article discusses the fundamentals of nasal reconstruction and describes the local and regional transposition flaps for the reconstruction of nasal defects.
Etiology
The challenge of nasal reconstruction is related to the complexity of the defect in an organ in which function, structural integrity, and contour are to be maintained. The differences in color, texture, and thickness between the nasal remnants and resources of skin available for the reconstruction pose aesthetic limits that are often difficult to overcome. The age, general health, and aesthetic goals of the patient should also be included in the decision-making process. These multifactorial problems can be approached with several reconstructive options, ranging from primary closure, healing by secondary intention, and skin grafting to the use of local or regional skin flaps. The decision as to which flap to use is based on a careful consideration of which tissue may be borrowed, how it can be repositioned, what the immediate- and long-term effects of moving that tissue will be, and how the scars may be hidden.
Flaps are the only reliable way to transfer bulk tissue for nasal reconstruction because their own source of nutrient blood makes them relatively independent of the vascularity of the recipient site for their survival. Flaps may therefore be used to cover nonvascular structures such as bare bone and cartilage. Nasal cutaneous flaps used to repair the nose provide excellent camouflage because of skin match in terms of texture, color, and thickness. Excess skin in the cephalic two-thirds of the nose can be moved into adjacent defects. The alar region is less suited for local transposition flaps or rotation flaps because the alar crease is often distorted or obliterated by the flap.
This article discusses the major principles of nasal reconstruction and describes the local and regional transposition flaps for the reconstruction of nasal defects.
Considerations in nasal reconstruction
Nasal units are covered by skin of a specific color, texture, and thickness. In addition, each unit has specific contours determined by soft and hard tissues. The decision-making process in reconstruction of nasal defects should include consideration of which tissue can be harvested for reconstruction, how it may be transferred to the nose, what the immediate- and long-term effects on the donor site will be, and how the scars may best be camouflaged. The nose must be restored to as normal appearing and functioning structure as possible. The following are the 3 principles that form the basis for this reconstructive process :
- 1.
Replace missing tissue with like tissue.
- 2.
Replace missing portions of the nasal skeleton with cartilage designed to precisely replicate the missing part.
- 3.
Divide the topography of the nose into aesthetic units for planning incisions and flaps. For units with convex contours (alae, tip, columella), resurface the entire unit with a skin flap if most of the skin of the unit is lost.
Replace Missing Tissue with Like Tissue
Nasal skin varies in texture, color, and appearance within different areas of the nose. The nasal dorsum, sidewalls, columella, alar margins, and soft triangles are covered with thin smooth skin. The nasal tip and ala are covered with thick pitted skin because of the presence of sebaceous glands. The color of the skin may vary from pale with a matt texture on the side of the nose to a shade of red-pink with a shiny appearance over the nasal tip.
In an attempt to replace nasal skin with like tissue, cheek flaps (unlike skin grafts) are especially useful in thick-skinned zones of the nose because medial cheek skin has similar color and texture. Paramedian forehead flaps are used to repair larger deeper defects because they provide sufficient surface area to completely cover the defect and provide adequate vascularity to support structural framework grafts. Loss of internal nasal lining should be restored with septal mucosa or adjacent vestibular skin.
Replace Missing Portions of the Nasal Skeleton
Loss of cartilage support because of removal of the upper or lower lateral cartilages should be restored by replacing the missing portions of the nasal skeleton with septal or auricular cartilage. Defects extending to the alar margin may result in retraction or partial collapse of the nostril if the ala is not properly supported with a batten in the form of a cartilage graft. Structural alar grafts are usually obtained from the contralateral conchal cartilage. These grafts are positioned between the lateral crura and alar base.
Alar batten grafts give support to and prevent retraction of the nostril margin and prevent constriction of the external nasal valve. Auricular cartilage is usually used to replace missing portions of the alar cartilages. Septal cartilage is typically used to replace the upper lateral cartilage. When bone is missing, it is usually replaced with cranial bone grafts or costal bone and cartilage grafts.
Aesthetic Units
Strategic incision placement
Although there is no control over wound healing, the surgeon can select flap donor sites with preferred skin color, texture, and thickness. The surgeon also has control over the size, configuration, and placement of incisions used to harvest and transfer skin flaps so that scars are most ideally located for maximal camouflage. Incisions are placed strategically so that they are parallel to relaxed skin tension lines (RSTLs) or are positioned at the junction of aesthetic facial regions ( Fig. 1 ). When possible, skin flaps are positioned so that their borders lie along the ridges and valleys of the nasal aesthetic units.
The unit principle
The aesthetic unit theory is important in nasal reconstruction. If a line of light or shadow (caused by scarring) crosses a smooth surface where it is not expected, it will be noticed at a glance ( Fig. 2 ). A good scar remains hidden from view because it is perceived visually as a normal facial fold or contour line. If a scar is placed between nasal topographic units, where it follows the join of normal lighted ridges and shallowed valleys, it will also be taken as normal. Equally important, the bulge of a flap caused by trapdoor contractions will mirror the normal contour of convex nasal units.
The aesthetic unit principle suggests that if a defect encompasses more than 50% of a unit, excision of the residual normal tissue should be considered ( Fig. 3 ). This way, the entire unit is reconstructed with a flap instead of patching the original defect. Resurfacing the entire nasal aesthetic unit may position scars in joints between the 3-dimensional units, where they may be hidden and less visible. This maneuver is most effective in the reconstruction of the convex units of the tip and alae, which are surrounded with fairly abrupt distinct borders. In these locations, the unit principle uses the trapdoor effect to re-create a 3-dimensional convexity because many flaps have a tendency to pincushion and stand as a bulge above the adjacent skin.
Considerations in nasal reconstruction
Nasal units are covered by skin of a specific color, texture, and thickness. In addition, each unit has specific contours determined by soft and hard tissues. The decision-making process in reconstruction of nasal defects should include consideration of which tissue can be harvested for reconstruction, how it may be transferred to the nose, what the immediate- and long-term effects on the donor site will be, and how the scars may best be camouflaged. The nose must be restored to as normal appearing and functioning structure as possible. The following are the 3 principles that form the basis for this reconstructive process :
- 1.
Replace missing tissue with like tissue.
- 2.
Replace missing portions of the nasal skeleton with cartilage designed to precisely replicate the missing part.
- 3.
Divide the topography of the nose into aesthetic units for planning incisions and flaps. For units with convex contours (alae, tip, columella), resurface the entire unit with a skin flap if most of the skin of the unit is lost.
Replace Missing Tissue with Like Tissue
Nasal skin varies in texture, color, and appearance within different areas of the nose. The nasal dorsum, sidewalls, columella, alar margins, and soft triangles are covered with thin smooth skin. The nasal tip and ala are covered with thick pitted skin because of the presence of sebaceous glands. The color of the skin may vary from pale with a matt texture on the side of the nose to a shade of red-pink with a shiny appearance over the nasal tip.
In an attempt to replace nasal skin with like tissue, cheek flaps (unlike skin grafts) are especially useful in thick-skinned zones of the nose because medial cheek skin has similar color and texture. Paramedian forehead flaps are used to repair larger deeper defects because they provide sufficient surface area to completely cover the defect and provide adequate vascularity to support structural framework grafts. Loss of internal nasal lining should be restored with septal mucosa or adjacent vestibular skin.
Replace Missing Portions of the Nasal Skeleton
Loss of cartilage support because of removal of the upper or lower lateral cartilages should be restored by replacing the missing portions of the nasal skeleton with septal or auricular cartilage. Defects extending to the alar margin may result in retraction or partial collapse of the nostril if the ala is not properly supported with a batten in the form of a cartilage graft. Structural alar grafts are usually obtained from the contralateral conchal cartilage. These grafts are positioned between the lateral crura and alar base.
Alar batten grafts give support to and prevent retraction of the nostril margin and prevent constriction of the external nasal valve. Auricular cartilage is usually used to replace missing portions of the alar cartilages. Septal cartilage is typically used to replace the upper lateral cartilage. When bone is missing, it is usually replaced with cranial bone grafts or costal bone and cartilage grafts.
Aesthetic Units
Strategic incision placement
Although there is no control over wound healing, the surgeon can select flap donor sites with preferred skin color, texture, and thickness. The surgeon also has control over the size, configuration, and placement of incisions used to harvest and transfer skin flaps so that scars are most ideally located for maximal camouflage. Incisions are placed strategically so that they are parallel to relaxed skin tension lines (RSTLs) or are positioned at the junction of aesthetic facial regions ( Fig. 1 ). When possible, skin flaps are positioned so that their borders lie along the ridges and valleys of the nasal aesthetic units.
The unit principle
The aesthetic unit theory is important in nasal reconstruction. If a line of light or shadow (caused by scarring) crosses a smooth surface where it is not expected, it will be noticed at a glance ( Fig. 2 ). A good scar remains hidden from view because it is perceived visually as a normal facial fold or contour line. If a scar is placed between nasal topographic units, where it follows the join of normal lighted ridges and shallowed valleys, it will also be taken as normal. Equally important, the bulge of a flap caused by trapdoor contractions will mirror the normal contour of convex nasal units.
The aesthetic unit principle suggests that if a defect encompasses more than 50% of a unit, excision of the residual normal tissue should be considered ( Fig. 3 ). This way, the entire unit is reconstructed with a flap instead of patching the original defect. Resurfacing the entire nasal aesthetic unit may position scars in joints between the 3-dimensional units, where they may be hidden and less visible. This maneuver is most effective in the reconstruction of the convex units of the tip and alae, which are surrounded with fairly abrupt distinct borders. In these locations, the unit principle uses the trapdoor effect to re-create a 3-dimensional convexity because many flaps have a tendency to pincushion and stand as a bulge above the adjacent skin.
Primary or delayed nasal reconstruction
Especially in the caudal third of the nose, there is an intimate attachment between skin and lower lateral cartilages such that invasion of the cartilage occurs relatively early in the course of the disease. Studies have shown that the highest percentages of recurrent basal cell carcinomas are nasal, illustrating the difficulty of tumor control in this area. This may be because of a tendency toward narrow excision margins in an effort to simplify reconstruction in this aesthetically important area and also because skin cancer of the midface is known to show subclinical tumor spread, which seems to be related to the embryonic fusion planes at this site. Skin cancer invades deeply along these planes rather than crossing the borders of fusion planes.
Primary reconstruction of nasal skin cancer defects is safe in most cases under the conditions of proper patient selection and reliable histopathologic examination techniques. Delay of reconstruction should be considered, sometimes even after Mohs surgery, if there is doubt about the completeness of the tumor resection. Particularly in large, recurrent, or aggressive skin tumors (eg, perineural growth, deep invasion of the bony or cartilaginous framework of the nose), the timing of reconstruction should be postponed until there is greater certainty that tumor regrowth has not occurred ( Fig. 4 ). Using a split- or full-thickness skin graft or allowing the wound to heal by secondary intention as an interim repair can offer surveillance for recurrence at the resected site.
Nasal reconstruction techniques
A variety of surgical techniques are available for reconstruction of the nose. The choice of technique is based on the size, depth, and location of the surgical wound as well as on the availability and condition of the surrounding tissue. Transposition flaps are reliable reconstructive tools for the reconstruction of nasal defects. A transposition flap is a random pattern skin flap that borrows skin from an adjacent area with relative skin laxity to fill a defect in an area with little or no skin laxity. When the flap is transferred from the donor site to the recipient site, it is lifted over a segment of intervening tissue following a rotational pathway. When properly executed, an excellent redistribution and redirection of tension can be achieved. One of the biggest advantages of transposition flaps is that these flaps use adjacent skin, which provides a good color and textural match. The authors provide an overview of the most important local and regional flaps for nasal reconstruction in the following sections.
Local Flaps
Rhomboid flap
The rhomboid flap optimizes the distribution of wound tension by orienting the flap design according to the lines of maximum extensibility (perpendicular to the RSTLs). However, the geometric design of the rhomboid flap (with 8 possible variations) prevents placement of all necessary incisions in or parallel to the RSTL or aesthetic boundary lines. The possible exception is the lateral nasal sidewall and the glabellar region ( Fig. 5 ).
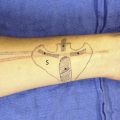
Note flap
An elegant alternative to a rhomboid flap is a note flap. This flap avoids the need to sacrifice normal tissue at the margins of a circular defect to create the geometric pattern that is required for a rhomboid flap. The note flap is in essence a triangular transposition flap, which is capable of closing a circular defect with little donor site deformity. The simplest form of the flap is depicted in Fig. 6 . It is extremely easy to design the flap in relation to the RSTL. For a circular defect, the surgeon draws 2 tangents approximately parallel to the RSTL of the nose. Then, 4 potential flaps are designed, and the surgeon selects the best of the 4 options. Ideally, the RSTL should parallel the final donor site wound closure line. One of the disadvantages of the note flap is that frequently there is a standing cutaneous deformity (SCD) at the base of the triangular flap, although usually no tailoring is required. A more important disadvantage is that the flap requires a certain degree of judgment based on experience. Because the note flap is somewhat smaller than the defect the surgeon must be sure that there is sufficient tissue laxity to allow wound closure.
Related posts:
 Melolabial Flaps for Nasal Reconstruction
Melolabial Flaps for Nasal Reconstruction
 Complex Nasal Reconstruction: A Case Study: Composite Defect
Complex Nasal Reconstruction: A Case Study: Composite Defect
 Complex Nasal Reconstruction: A Case Study: Reconstruction of Full-Thickness Nasal Defect
Complex Nasal Reconstruction: A Case Study: Reconstruction of Full-Thickness Nasal Defect
 Reconstruction of the Dorsal and Sidewall Defects
Reconstruction of the Dorsal and Sidewall Defects
 Reconstruction of Nasal Tip and Columella
Reconstruction of Nasal Tip and Columella
 Microvascular Reconstruction of Nasal Defects
Microvascular Reconstruction of Nasal Defects
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


