Key points
- •
Preseptal, preperiosteal transconjunctival approach.
- •
Low risk of postoperative lower eyelid malposition.
- •
Low risk of facial nerve injury.
- •
Restoration and reinforcement of proper lateral canthal position.
- •
Improvement of tear trough deformity.
- •
Reduced post-operative recovery.
Introduction
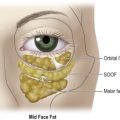
Rejuvenation of the midface remains a challenging aesthetic area to obtain natural looking, safe, and long-lasting results. The periorbital region ages in a predictable fashion ( Figure 13.1 ). The brow, the upper eyelid, and the lower eyelid/midface age in a composite fashion. The brow apex tends to flatten and drop with aging as the forehead becomes variably redundant. The upper eyelid soft tissue becomes redundant with involutional changes caused by deflation. The lateral canthal complex moves inferiorly in varying degrees, leading to loosening of the lower eyelid sling and elongation of the lower eyelid. Finally, as the midface migrates inferiorly, the tear trough becomes visible and the jowl becomes increasingly prominent.

Additional important features of aging include elongation of the suspensory ligaments that result in descent of the malar fat pad and cheek skin. This change effectively skeletonizes the infraorbital rim, deepens the tear trough and exaggerates the nasolabial fold. Subtle effects like scleral show and lower eyelid elongation are secondary to lengthening and thinning of the orbicularis oculi. Vertical suspension of the malar fat pad and cheek skin are required to counteract the downward displacement of gravity. Secondary benefits include restoration of youthful convexity of the malar contour and vertical decrease of the distance from the lid to the lid/cheek junction.
Multiple fibrous ligaments provide support and restrict the movement of lower eyelid skin, orbicularis, malar fat pad and SMAS, collectively called the midface. Several orbicularis retaining ligaments attach the orbicularis to the inferior orbital rim. The lateral orbital thickening is a triangular condensation of superficial and deep fascia that attaches the orbicularis to the frontal process of the zygoma and the lateral canthal tendon. The zygomaticofacial ligaments fix the malar fat pad and cheek skin to the underlying zygomatic eminence. Attenuation of these attachments contributes to the typical aging changes in the midface. Release allows effective redraping and upward mobilization of the orbicularis of the lower lid and the premalar soft tissues.
Much has been done in the area of midface rejuvenation over the past decade. Innovators such as Dr Flowers, Dr Hester, and Dr Paul are a few of the well-known names in this arena. These surgeons have learned many of the difficult lessons for midface rejuvenation and were willing to share their findings with the rest of us. Dr Flowers emphasized the importance of looking at the forehead, upper eyelid, and lower eyelid–midface together when considering treatment, giving rise to his ‘coronocanthoplasty procedure’. He introduced the importance of drill hole fixation for midface elevation. This concept is particularly important to avoid crowding of the temporal area in midfacial elevation. In addition, correction of the midface alone leads to unnatural results in most cases.
Dr Hester is credited with the introduction of the subciliary, skin–muscle flap approach to the midface lift. He performed many such procedures successfully, but also was willing to share his complications. In particular, he showed the importance of lower lid support in the form of canthopexy or canthoplasty. Dr Hester proved that the lower lid alone is not enough to support an aggressive midface lift; multiple points and reliable suture fixation are vital. He went on to suggest that conservative or delayed skin resection should be considered for the lower eyelid during midface lifting. Dr Jelks has introduced principles that have significant relevance in midfacial rejuvenation. The ‘no touch technique’ for lower blepharoplasty incorporates the concept of avoiding surgical trauma to the orbicularis oculi, especially the pretarsal aspect. He has shown a number of examples where lower lid paralysis leads to significant lid malposition. He has also shown that the middle lamella is extremely susceptible to inflammation and fibrosis, with blood in the middle lamella and lid laxity being the perfect combination for lower lid retraction. A transconjuctival approach divides the lower lid retractor, the capsulopalpebral fascia, while preserving the muscle and underlying muscle fascia. The addition of the lateral retinacular suspension adds a significant barrier to lower lid malposition. Ultimately, what these investigators have shown is that proactive lid position protection is vital before considering the aesthetic result, as the lower lid is the Bermuda Triangle of facial rejuvenation.
Our experience with transconjunctival deep plane midface lifting began in patients who suffered complications with the more traditional midface rejuvenation techniques. These were patients with severe ectropion, lid paralysis, and unacceptable cosmetic outcomes. In an effort to consider a less invasive or less traumatic approach, the transconjunctival approach was born. Our experience allowed for the recruitment of more than 2 cm of skin, while avoiding the need for lower lid skin grafts. This technique could be combined with a formal canthoplasty or lateral tarsal strip procedure, while minimizing temporary or permanent orbicularis paresis. Our approach led to dramatic corrections without recurrence of the original lid malposition. Ultimately, the technique, which will be outlined in greater detail below, found its place in primary cases.
The various planes of dissection within the cheek region have led to the development of multiple techniques for midface lifting. While many of these approaches are very safe and effective in skilled hands, extensive subperiosteal dissection and surgical manipulation of the lower eyelid/cheek junction can be unforgiving. Periosteal tissue is rich in lympathics, and their disruption leads to increased edema, and potentially prolonged post-operative chemosis and midfacial edema. Periorbital swelling may also contribute to malpostioning of the lower eyelid by creating a downward pull on the lower eyelid and lateral canthus. The transconjunctival deep plane midface lift avoids most of the above issues, giving the surgeon a consistent approach. Our approach is relatively easy to apply with minimal risk and significant benefit. We feel that the combination of transconjunctival exposure and preservation of the periosteum results in significantly less post-operative morbidity.
Patient selection
Our technique can be performed on most patients desiring periorbital rejuvenation, with an emphasis on the lower eyelid–cheek junction. The transconjunctival deep plane midface lift was initially designed to treat those individuals with a higher risk eye exam, including vector-negative patients. We found that preservation of the orbicularis was a vital component of the minimization of postoperative risk. While the technique minimizes risk during midfacial rejuvenation, it is vital to survey patients for risk factors in order to prepare the patient for potential limitations of the intervention. The patient with a shallow orbit or vector negative exam is the highest risk patient for any form of periorbital surgery. The transconjunctival deep plane midface lift is ideal in this patient population. One must also consider lid laxity, canthal malposition, and previous skin or deep tissue trauma before operation, as the patient will require special consideration. The patient with more than 6–8 mm of lower lid distraction should be considered for formal canthoplasty with possible tarsal strip procedure. A general medical and ophthalmologic history and physical examination must be well documented. Preoperative clinical photography is also essential in documenting existing anatomy and asymmetries. Risk factors for potential complications are listed in Box 13.1 . Patients presenting with malar bags and festoons are poor candidates for a transconjunctival procedure as they are more likely to have residual bags after transconjunctival deep plane midface lift. The patient with prominent malar excess is best served by more traditional skin muscle flap surgery with canthoplasty, as well described by Hester, McCord, Codner, and Nahai. Another approach for the patient with prominent festoons has been either direct excision or laser resurfacing combined with the transconjunctival deep plane midface lift procedure.
- •
Shallow orbit.
- •
Proptotic globe.
- •
Lid laxity.
- •
Scleral show.
- •
Canthal malposition.
- •
Previous laser/skin treatment.
- •
Blepharoptosis.
- •
History of trauma or surgery.
- •
Neurologic syndrome.
- •
Significant anatomic asymmetry.
Indications
The lower eyelid and midface function as an aesthetic unit. Therefore, a comprehensive evaluation of a patient undergoing periorbital rejuvenation must include examination of the brow, upper eyelid, lower eyelid–cheek junction, and midface–jowl. Clinically, aging of the lower eyelid and midface unit is not an isolated event and presents with the following: descent of the cheek fat pad with laxity of the orbitomalar ligament, inferior migration of the lateral canthus/commissure, descent of the lid–cheek junction, laxity and descent of the orbicularis muscle, and deepening of the tear trough (nasojugal groove) deformity.
Although the aging process is largely characterized by descent and laxity of periorbital structures, volume loss is also a significant factor. Our approach to periorbital rejuvenation not only addresses the need for resuspension of structures, but it can be complemented with such techniques as autogenous fat grafting for volume replacement.
Special consideration: correction of the ectropion patient
The transconjunctival deep plane midface procedure was first successfully used to treat patients with cicatricial ectropions. The techniques, as described, are ideal for ectropion treatment for the following reasons. This approach avoids direct trauma to the orbicularis, sparing potential weakness that could contribute to recurrence. The lower lid retractor, also known as the capsulopalpebral fascia, is divided by the transconjunctival approach and we consciously do not reapproximate the layer. By preserving the muscle and deactivating an important lid retractor, the odds of success increase while limiting morbidity, excessive edema being the most significant. This approach also lends itself to the use of the transconjunctival spacer grafts (AlloDerm® or Enduragen™ are preferred), for patients with middle lamellar scarring ( Figure 13.2 ). The inset is not complicated, with the use of 5-0 fast absorbing suture or 6-0 vicryl. Figures 13.8 illustrates this indication, with the treatment of a left sided ectropion after subciliary incision placed for orbital fracture repair. We routinely use a lateral suture tarsorrhaphy in these cases, removing them at 5–10 days, depending on the case and postoperative edema. This approach can be used in patients with prior conjunctival or cutaneous incisions.

Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 No touch lower blepharoplasty
No touch lower blepharoplasty
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


