The author presents his procedure for neck rejuvenation using a modified Fogli approach, which involves a transverse incision in Loré’s fascia in the pretragal region, a “take-down” of the auriculoplatysmal ligament by resection to the body of the platysma where it crosses the sternomastoid muscle and then a triple cable suture fixation to the cut edge of Loré’s fascia. Platysma bands are assessed for their degree of redundancy and those judged excessive in thickness or descent are resected via a submental incision. A strong, permanent elevation of the middle and the lower third of the platysma is achieved.
Key points
- •
Once understood that Loré’s fascia was really a thickening of the parotid fascia in the pretragal region and that fascia descended down in front of the facial nerve attaching to the styloid process and the tympanic fissure, it became clear that this skull-based stout ligament had adequate strength to support the traction of the tissues in a permanent way.
- •
Platysma bands, once resected, do not recur but if observed laterally on animation and found to be disconcerting to the patient, can be treated with botulinum toxin A injections.
- •
Unfurling of the horizontal wrinkles and the tightening of loose lower neck skin results in a “tallness” of the neck that is best achieved by addressing the entire sternomastoid from the suprasternal region to up behind the angle of the mandible.
Editor Commentary: I have known and I have traded thoughts and concepts with Darryl Hodgkinson for many years. In his chapter, he describes how he has evolved in his management of the platysma muscle including modifying the Fogli technique. Addressing the full vertical height of the platysma muscle as well as correcting horizontal aging changes in the appearance of the neck are important advances in approaching the common problems that often diminish the overall result when not addressed.
Introduction
Over the past 6 years the author has modified his approach to the aging neck by directing his attention to resecting the redundant platysmal bands after strong superior traction of the body of the platysma muscle to the temporoparotid fascia (Loré’s fascia) instead of suturing medial platysmal bands. This technique is a variation of Fogli’s initial description, the main difference being that the elevation of the platysma is achieved by a triple cable braided 2/0 suture to the cut edge of Loré’s fascia in front of the tragus, affording a strong, permanent elevation of the middle and the lower third of the platysma as well as a horizontal vector. If the horizontal vector is inadequate to improve the jawline in the submental area, a separate submental incision is made to approach the muscles. When this occurs, the redundant muscle bands are resected, not sutured together.
Introduction
Over the past 6 years the author has modified his approach to the aging neck by directing his attention to resecting the redundant platysmal bands after strong superior traction of the body of the platysma muscle to the temporoparotid fascia (Loré’s fascia) instead of suturing medial platysmal bands. This technique is a variation of Fogli’s initial description, the main difference being that the elevation of the platysma is achieved by a triple cable braided 2/0 suture to the cut edge of Loré’s fascia in front of the tragus, affording a strong, permanent elevation of the middle and the lower third of the platysma as well as a horizontal vector. If the horizontal vector is inadequate to improve the jawline in the submental area, a separate submental incision is made to approach the muscles. When this occurs, the redundant muscle bands are resected, not sutured together.
Aesthetics and history
A tall, well-toned, and distinctly defined neck is synonymous with youth and beauty. Most surgical procedures have focused solely on the upper neck and jaw, improving the definition of the cervicomental angle.
When the author began to perform facelifting procedures in the late 1970s, he was profoundly influenced by Dr Bruce Connell’s and others’ work in the variety of platysmaplasties that aimed to achieve long-term results in neck rejuvenation. The author used the principles of transection and posterior traction of the platysma for many years. He also incorporated in his technique the work of many authors of the 1980s and 1990s, who manipulated, sutured, transected, and plicated the anterior platysmal bands via the submental incision. The unfortunate recurrence of platysmal bands and associated patient dissatisfaction with the result in the lower neck, especially around the suprasternal notch, was a persistent concern. The author was influenced by Dr Alain Fogli’s presentations in 2005 when he published the strong, vertical elevation of the platysma muscle, affixing it to Loré’s fascia. The author then began to adopt this maneuver and continued to modify his technique over the subsequent 6 years. His concept has changed to include the rejuvenation of the entire neck from the clavicles to the mastoid region: defining the jawline and the sternomastoid muscle, reducing horizontal wrinkling in the neck, unfurling the neck, and giving the neck the visual appearance of increased height and tone.
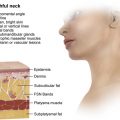
Initially Loré’s fascia seemed to be an elusive anatomic structure. Once understood, however, that it was really a thickening of the parotid fascia in the pretragal region and that fascia descended down in front of the facial nerve attaching to the styloid process and the tympanic fissure, it was appreciated that this skull-based stout ligament had adequate strength to support the traction of the tissues in a permanent way ( Fig. 1 ).
The anatomic and functional platysma
In 1865, Duchenne demonstrated isolated platysmal contraction by electrophysiological stimulation, which showed that the middle third of the platysma muscle was responsible for horizontal neck wrinkles, shortening, and tightening of the skin across the clavicle as well as a drawing down of the lower lip and mandible.
The trapezoidal-shaped platysma muscles pass obliquely from the mandible, crossing the sternomastoid to insert in the skin of the upper chest. Most of the muscles’ weight is therefore situated in the lower half of the neck. The 2 plastymal muscles both attach at the mentum, however, with varying degrees of divarication and fascial attachment. As the muscles pass over the mandible, there are fascial attachments of the platysmas to the ramus of the mandible that on contraction lead to an inferior movement of the lower jaw.
The platysma muscles may be quite lax with virtually no motor innervations, dynamic in nature, or spasmodic. Before surgery, the tone in the platysma muscles must be ascertained to determine which bands need to be resected, which bands can be surgically ignored, and which bands can be retracted significantly enough via the described muscle fixation to Loré’s fascia.
Clinical evaluation of the platysma
The patient is asked to contract the platysma muscle by grimacing ( Fig. 2 ).
The point where the platsyma crosses the anterior border of the sternomastoid is marked.
The anterior border of the platysma is evaluated for thickness and descent ( Fig. 3 ).
Related posts:
 Nonexcisional, Minimally Invasive Rejuvenation of the Neck
Nonexcisional, Minimally Invasive Rejuvenation of the Neck
 Progressive Tunnelizations in Neck Face Lift Detachment
Lore’s Fascia a Strong Fixation Point for Neck Rejuvenation Procedures
Progressive Tunnelizations in Neck Face Lift Detachment
Lore’s Fascia a Strong Fixation Point for Neck Rejuvenation Procedures
 Managing the Components of the Aging Neck
Managing the Components of the Aging Neck
 Multidimensional Evaluation and Surgical Approaches to Neck Rejuvenation
Multidimensional Evaluation and Surgical Approaches to Neck Rejuvenation
 Neck Lift Technique
Neck Lift Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


