At less than 90 degrees of active knee flexion, a total knee arthroplasty (TKA) has inadequate range of motion (ROM) for performing many activities of daily living. The required ROM for daily activities are as follows4,12:
Sixty-seven degrees of flexion for normal gait on level ground
Eighty-three degrees of flexion to climb stairs
Ninety to 100 degrees of flexion to descend stairs
Ninety-three degrees of flexion to stand from a standard-height chair
One hundred five degrees of flexion to tie a shoe
 Flexion contractures can be equally disabling: A flexion contracture of more than 15 degrees is usually considered pathologic because it greatly inhibits normal gait.
Flexion contractures can be equally disabling: A flexion contracture of more than 15 degrees is usually considered pathologic because it greatly inhibits normal gait.
ANATOMY
 The primary impediments to exposure of the revision TKA, particularly a stiff TKA, are the extensor mechanism and the patella. The exposure can be thought of as a progressive release or “unleashing” of the extensor mechanism.
The primary impediments to exposure of the revision TKA, particularly a stiff TKA, are the extensor mechanism and the patella. The exposure can be thought of as a progressive release or “unleashing” of the extensor mechanism.
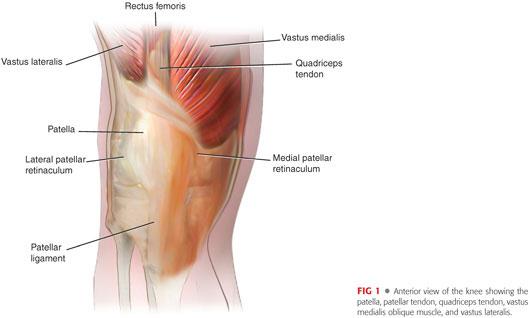
 The four tethers of the extensor mechanism (FIG 1) are the following:
The four tethers of the extensor mechanism (FIG 1) are the following:
Proximal: quadriceps tendon and musculature
Medial: medial joint capsule and retinaculum with the insertion of the vastus medialis
Lateral: lateral joint capsule and retinaculum with the insertion of the vastus lateralis
Distal: patellar tendon
 The blood supply to the patella is provided by an anastomotic ring of vessels supplied by the geniculate arteries. It is important to try to avoid complete devascularization of the patella because avascular necrosis can occur.
The blood supply to the patella is provided by an anastomotic ring of vessels supplied by the geniculate arteries. It is important to try to avoid complete devascularization of the patella because avascular necrosis can occur.
 The blood supply to the skin overlying the knee travels from the deeper tissues up through the superficial fascia and does not run superficially. If skin flaps are required at the time of surgery, they must be full thickness to avoid skin necrosis.
The blood supply to the skin overlying the knee travels from the deeper tissues up through the superficial fascia and does not run superficially. If skin flaps are required at the time of surgery, they must be full thickness to avoid skin necrosis.
PATHOGENESIS
 Many potential causes for stiffness following TKA exist and multiple mechanisms may act in concert in a given patient, resulting in suboptimal ROM.
Many potential causes for stiffness following TKA exist and multiple mechanisms may act in concert in a given patient, resulting in suboptimal ROM.
 Poor perioperative pain control or suboptimal physical therapy. In rare cases, a chronic regional pain syndrome develops, characterized by severe pain, cutaneous hypersensitivity, vasomotor disturbance, and stiffness.
Poor perioperative pain control or suboptimal physical therapy. In rare cases, a chronic regional pain syndrome develops, characterized by severe pain, cutaneous hypersensitivity, vasomotor disturbance, and stiffness.
 Technical issues related to the original surgical procedure may play a role.
Technical issues related to the original surgical procedure may play a role.
Femoral component
• Oversized: leads to tightness in flexion
• Internally rotated: leads to patellar maltracking or an asymmetric flexion gap
• Inadequate distal femoral resection: leads to tightness in extension and a potential flexion contracture, or alternatively, a knee that is stable in extension but loose in flexion
• Overresection of the distal femur: requires a thicker polyethylene insert to obtain stability in extension, thereby leading to tightness in flexion
• Inadequate removal of posterior femoral osteophytes: leads to tenting of the posterior capsule and flexion contracture or osteophytes that can impinge on the tibial polyethylene insert, limiting flexion
• Anterior placement of the femoral component: can lead to “overstuffing” of the patellofemoral joint
Tibial component
• Most commonly, inadequate or reverse slope of the tibial cut, which leads to tightness in flexion
• Internal rotation of the tibial component, which leads to patellar maltracking
• Oversized tibial component, which can lead to soft tissue impingement and pain
• Inadequate resection of the tibia: leads to tightness in both flexion and extension
Patellar component
• Under-resection of the patella: can lead to overstuffing of the patellofemoral articulation. The native patella–prosthetic composite in most cases should be equivalent in thickness to the patella before resection.
• Excessive patellar resection: leads to weakness of the extensor mechanism with initial extensor lag and eventual flexion contracture
• Inadequate medialization of the component: can lead to patellar maltracking
• Inadequate removal of lateral patellar osteophytes: can lead to impingement and pain
Ligamentous imbalance: flexion–extension mismatch (typically too tight in flexion, particularly with a cruciate-sparing design) or varus–valgus instability
Elevation of the joint line (particularly if >1 cm): leads to poor ROM secondary to altered patellofemoral joint mechanics
Poor component fixation: failed ingrowth of cementless components or inadequate cement mantle around cemented components, resulting in persistent pain that inhibits physiotherapy
 Patient-related factors
Patient-related factors
Poor preoperative ROM (the best predictor of postoperative ROM is preoperative ROM)
Genetic predisposition to scarring and stiffness
A history of previous surgery on the knee that has led to stiffness or a patella baja (shortening of the patellar tendon)
Noncompliance with physical therapy
Obesity (soft tissue envelope of the posterior thigh and leg limits flexion)
Stiffness or arthritis of the ipsilateral hip
 Deep infection must always be considered in the differential diagnosis.
Deep infection must always be considered in the differential diagnosis.
 Heterotopic ossification
Heterotopic ossification
NATURAL HISTORY
 The natural history of stiff TKA is poor. Even with time, patients’ ROM rarely improves enough to positively impact their gait pattern, and chronic pain develops.
The natural history of stiff TKA is poor. Even with time, patients’ ROM rarely improves enough to positively impact their gait pattern, and chronic pain develops.
 Flexion contractures are equally poorly tolerated. Flexion contractures greater than 15 degrees limit the ability to stand up straight and cause substantial fatigue when walking.
Flexion contractures are equally poorly tolerated. Flexion contractures greater than 15 degrees limit the ability to stand up straight and cause substantial fatigue when walking.
 Patients with only mild stiffness (ie, ROM near 90 degrees) may improve slightly (5 to 10 degrees) in the first 2 years after surgery, reaching a level of flexion that is tolerable for most activities of daily living.
Patients with only mild stiffness (ie, ROM near 90 degrees) may improve slightly (5 to 10 degrees) in the first 2 years after surgery, reaching a level of flexion that is tolerable for most activities of daily living.
PATIENT HISTORY AND PHYSICAL FINDINGS
 The history is a critical part of the evaluation to determine which of the factors listed under Pathogenesis have led to stiffness; in most cases, more than one factor is at work.
The history is a critical part of the evaluation to determine which of the factors listed under Pathogenesis have led to stiffness; in most cases, more than one factor is at work.
 Direct questions should be asked to determine whether pain control was adequate in the postoperative period.
Direct questions should be asked to determine whether pain control was adequate in the postoperative period.
Did the patient have severe pain postoperatively that limited his or her ability to perform physical therapy?
For how long postoperatively did the patient require narcotics? Is the patient still taking narcotics and still in severe pain?
Does the patient have hypersensitivity of the skin overlying the incision or other complaints that suggest neurogenic pain or a chronic regional pain syndrome?
How was the patient’s stiffness addressed postoperatively?
• Did he or she undergo a manipulation under anesthesia (MUA) postoperatively?
• Has he or she undergone any other operative procedures (eg, open or arthroscopic release) in an attempt to improve ROM?
Does any element of the history suggest infection?
• Wound drainage that persisted for more than a few days after surgery
• The use of antibiotics for more than 24 hours postoperatively
• Persistent pain that is of a different character than the pain the patient had before the surgery
Inspect the skin for the presence of a past or present sinus, indicating infection. Densely adherent skin is much harder to close and may represent a higher risk for necrosis and requires attention from a plastic surgeon.
Evaluate the patient’s ROM. Flexion of less than 90 degrees and a flexion contracture of more than 15 degrees are considered pathologic. Loss of ROM affects gait and ability to perform activities of daily living.
IMAGING AND OTHER DIAGNOSTIC STUDIES
 Standing anteroposterior, lateral, and patellar radiographs should be obtained to identify component loosening, malposition, or improper sizing (FIG 2A).
Standing anteroposterior, lateral, and patellar radiographs should be obtained to identify component loosening, malposition, or improper sizing (FIG 2A).
Patella baja and joint line position also should be noted (FIG 2B). Severe ligamentous imbalance may be readily apparent on the plain radiographs. Patellar maltracking can also be identified (FIG 2C), as can an unresurfaced patella, which may cause pain that leads to stiffness.
Serial radiographs often are helpful in confirming component loosening.
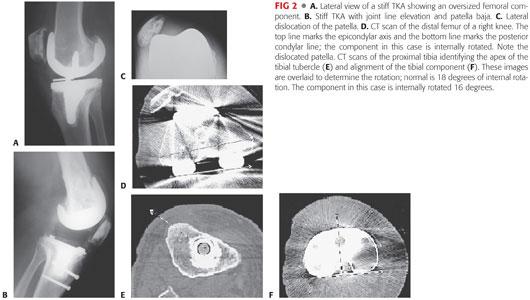
 A computed tomography (CT) scan to determine femoral and tibial component rotation is often performed (FIG 2D–F). If component malposition is identified (eg, internal rotation), the components are revised.3
A computed tomography (CT) scan to determine femoral and tibial component rotation is often performed (FIG 2D–F). If component malposition is identified (eg, internal rotation), the components are revised.3
 Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are obtained before every revision TKA.
Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level are obtained before every revision TKA.
If either is elevated, or if the history is very suspicious for an infection, an aspiration of the knee joint is obtained and sent for a cell count with differential and cultures. A synovial fluid white blood cell count above 3000 WBC/μL is considered consistent with infection, as is a differential of greater than 80% neutrophils.
Patients must have been off antibiotics for at least 2 weeks before the knee aspiration to avoid falsely negative cultures.
 At the time of revision, additional tissue or fluid cultures are taken from within the joint and an intraoperative frozen section is taken from the synovial tissues. An average of more than 10 polymorphonuclear cells identified within tissue (and not fibrin) is consistent with infection.
At the time of revision, additional tissue or fluid cultures are taken from within the joint and an intraoperative frozen section is taken from the synovial tissues. An average of more than 10 polymorphonuclear cells identified within tissue (and not fibrin) is consistent with infection.
 Nuclear medicine studies, such as a triple-phase bone scan, are occasionally helpful in identifying subtle loosening but are not routinely obtained.
Nuclear medicine studies, such as a triple-phase bone scan, are occasionally helpful in identifying subtle loosening but are not routinely obtained.
DIFFERENTIAL DIAGNOSIS
 Deep infection
Deep infection
 Component malposition (eg, internal rotation of the femur or tibia)
Component malposition (eg, internal rotation of the femur or tibia)
 Patellar maltracking or overstuffing of the patellofemoral joint
Patellar maltracking or overstuffing of the patellofemoral joint
 Improper component sizing
Improper component sizing
 Ligamentous imbalance (eg, tightness in flexion)
Ligamentous imbalance (eg, tightness in flexion)
 Component loosening
Component loosening
 Chronic regional pain syndrome
Chronic regional pain syndrome
NONOPERATIVE MANAGEMENT
 If the patient is seen early in the postoperative period (<6 to 12 weeks postoperatively), he or she can be managed with a combination of the approaches discussed in this section.
If the patient is seen early in the postoperative period (<6 to 12 weeks postoperatively), he or she can be managed with a combination of the approaches discussed in this section.
 Aggressive pain management, supervised by a physician with expertise in this area—usually an anesthesiologist who specializes in pain management
Aggressive pain management, supervised by a physician with expertise in this area—usually an anesthesiologist who specializes in pain management
If chronic regional pain syndrome is considered, a sympathetic blockade is often administered.
Intensive physical therapy, stressing active and passive ROM exercises
In cases of flexion contracture, dynamic splinting or the use of serial casts can be tried in an attempt to obtain full extension
 MUA can also be performed. When performing an MUA, the author prefers to place an indwelling epidural catheter at the same time, which will remain in place for several weeks after the procedure to assist with administration of medication for pain control. Patients are sent home with a pump to administer the medication and are carefully monitored by a pain control specialist.
MUA can also be performed. When performing an MUA, the author prefers to place an indwelling epidural catheter at the same time, which will remain in place for several weeks after the procedure to assist with administration of medication for pain control. Patients are sent home with a pump to administer the medication and are carefully monitored by a pain control specialist.
MUA seems to be most effective and is associated with a lower rate of complications (eg, periprosthetic fracture) if performed within 3 months of the index procedure.
The literature is unclear as to the magnitude of benefit derived. Most studies show that patients improve after MUA, but that their final ROM is less than that of their nonmanipulated counterparts.
Other potential complications of MUA include rupture of the patellar or quadriceps tendon, periprosthetic fracture of the femur or tibia, and wound dehiscence. The manipulation should be performed using a short-lever arm with the patient completely relaxed until a firm end point is reached. X-rays should be obtained following the manipulation to ensure that a fracture has not occurred.
SURGICAL MANAGEMENT
 The decision to proceed with revision TKA for stiffness should be considered carefully and only after a full investigation as to the cause or causes of stiffness. The patient must be fully informed of the risks of the procedure and that the ROM may not improve, even with further surgery. It is crucial to work with a pain management specialist and a physical therapist to ensure that stiffness does not recur postoperatively.
The decision to proceed with revision TKA for stiffness should be considered carefully and only after a full investigation as to the cause or causes of stiffness. The patient must be fully informed of the risks of the procedure and that the ROM may not improve, even with further surgery. It is crucial to work with a pain management specialist and a physical therapist to ensure that stiffness does not recur postoperatively.
 Options for surgical management include the following:
Options for surgical management include the following:
Arthroscopic débridement with manipulation2,5,7,15
• This can be performed in patients with well-fixed, appropriately aligned components. The procedure is technically demanding and the results reported in the literature are variable, with most studies showing mild improvements in ROM (15 to 30 degrees, on average).
• The technique includes release of the posterior cruciate ligament (if present), clearing of scar from the suprapatellar region, and typically MUA once the scar has been cleared.
• Flexion contractures are harder to address arthroscopically, but a posterior release can be performed using small, open, medial and lateral incisions.
Open arthrolysis with exchange of the modular polyethylene liner.1,9,10,13
• This procedure can also be performed in selected patients with well-fixed, appropriately aligned components. However, it often is difficult to fully release the posterior capsule to treat flexion contractures, and it is unclear whether this technique has any benefit over arthroscopic release. This option should be performed rarely.
Revision TKA6,8,10,11,14
• Revision TKA is the most appropriate treatment for most patients. It allows for optimization of component alignment, size, and rotation while providing the opportunity to restore the joint line and optimize ligamentous balance.
• It affords complete access to the posterior capsule to perform a capsulectomy and remove any retained osteophytes from the previous surgical procedure.
• An additional benefit is the option of using a more constrained polyethylene insert, if desired, to optimize stability if extensive releases are performed.
• If a large flexion contracture is being addressed, a flexion–extension mismatch often is present (ie, extension space smaller than the flexion space) and constrained and even hinged implants may be required.
Preoperative Planning
 The history, physical examination, plain radiographs, and CT scan (if obtained) are reviewed before a definite decision is made whether the components are to be removed or retained.
The history, physical examination, plain radiographs, and CT scan (if obtained) are reviewed before a definite decision is made whether the components are to be removed or retained.
 The ESR, CRP, synovial fluid white blood cell count with differential, and culture results are reviewed to determine whether a deep infection is present.
The ESR, CRP, synovial fluid white blood cell count with differential, and culture results are reviewed to determine whether a deep infection is present.
 If any of the prosthetic components are to be retained, the operative note from the previous procedure must be reviewed to definitely identify manufacturer, model, and size so that appropriate matching replacement implants and trials are available on the day of surgery.
If any of the prosthetic components are to be retained, the operative note from the previous procedure must be reviewed to definitely identify manufacturer, model, and size so that appropriate matching replacement implants and trials are available on the day of surgery.
 An examination under anesthesia confirms the limits of motion.
An examination under anesthesia confirms the limits of motion.
Positioning
 The operative extremity is draped free from the hip to the ankle and a tourniquet is placed on the upper thigh.
The operative extremity is draped free from the hip to the ankle and a tourniquet is placed on the upper thigh.
 A bump, placed underneath the ipsilateral hip, assists in keeping the leg upright.
A bump, placed underneath the ipsilateral hip, assists in keeping the leg upright.
 A leg holder keeps the leg in the desired position for surgery.
A leg holder keeps the leg in the desired position for surgery.
 An elastic bandage placed on the lower leg defines the malleoli, which are used as a reference for tibial cut alignment (FIG 3).
An elastic bandage placed on the lower leg defines the malleoli, which are used as a reference for tibial cut alignment (FIG 3).

Approach
 The workhorse method for exposure in revision TKA is the medial parapatellar approach with complete excision of intra-articular scar tissue. This approach is useful for most revision TKAs.
The workhorse method for exposure in revision TKA is the medial parapatellar approach with complete excision of intra-articular scar tissue. This approach is useful for most revision TKAs.
In the stiff knee, however, a more extensile approach may be required.
 If additional exposure is needed, a quadriceps snip can be performed.
If additional exposure is needed, a quadriceps snip can be performed.
This maneuver assists in freeing the proximal tether of the extensor mechanism, thereby improving exposure.
Benefits include relative simplicity of performance and repair, no need to alter postoperative rehabilitation protocols, and clinical results that have been shown to be equivalent to those in patients who have undergone a revision TKA without a snip.
 If a more extensile exposure is needed, the extensor mechanism can be completely released proximally with a V-Y quadricepsplasty (see Chap. 45) or distally with a tibial tubercle osteotomy (see Chap. 44). However, these maneuvers may be rarely required, and as their performance may in many cases lead to limitations in postoperative physical therapy, they should be avoided if possible when revising the stiff TKA.
If a more extensile exposure is needed, the extensor mechanism can be completely released proximally with a V-Y quadricepsplasty (see Chap. 45) or distally with a tibial tubercle osteotomy (see Chap. 44). However, these maneuvers may be rarely required, and as their performance may in many cases lead to limitations in postoperative physical therapy, they should be avoided if possible when revising the stiff TKA.
TECHNIQUES
 Medial Parapatellar Arthrotomy with Complete Intra-articular Release
Medial Parapatellar Arthrotomy with Complete Intra-articular Release
Skin incision
Previous skin incisions are used whenever possible.
Avoid parallel incisions. If choosing among multiple previous incisions, the most lateral one is selected because the blood supply is derived predominantly from the medial side.
Full-thickness flaps are raised, if required.
The arthrotomy extends from the apex of the quadriceps tendon, around the medial aspect of the patella and just medial to the tibial tubercle (TECH FIG 1A).
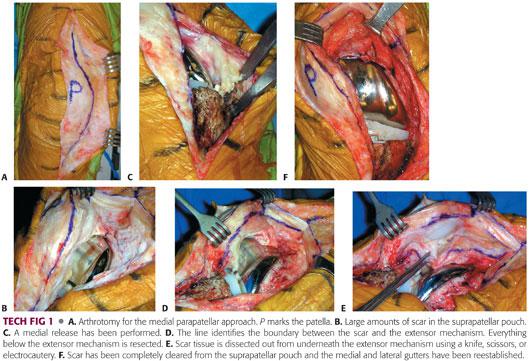
On entering the joint, large amounts of scar are typically encountered (TECH FIG 1B); these prevent proper exposure and contribute to stiffness.
A medial release is performed with electrocautery by subperiosteally releasing a continuous soft tissue sleeve all the way to the posteromedial corner of the tibia and the semimembranous insertion (TECH FIG 1C).
This allows for external rotation of the tibia, which relaxes the extensor mechanism and improves exposure.
The junction between scar and the extensor mechanism is identified (TECH FIG 1D). The scar is meticulously removed from underneath the extensor mechanism laterally (TECH FIG 1E) and from underneath the joint capsule medially until the medial and lateral gutters have been reestablished (TECH FIG 1F).
A thin layer of soft tissue is left on the distal femur to prevent excessive bleeding and the extensor mechanism from becoming readherent in this area.
The scar tissue is carefully cleared from the interval between the patellar tendon and the scar behind it to release it from the proximal tibia.
At this point, the modular polyethylene liner is removed to allow for patellar eversion or subluxation. In most cases, patellar subluxation is preferred because it places less tension on the extensor mechanism and provides adequate exposure in most cases.
If difficulty is encountered, soft tissue can be peeled off the lateral border of the patella to make it more mobile, and any osteophytes that are present can be removed.
If exposure still cannot be accomplished, a formal lateral retinacular release may be required.
This release involves a full-thickness division of the capsule along the lateral border of the patella from the proximal tibia (just lateral to the patella tendon) to the vastus lateralis.
A lateral release performed from the inside out eliminates the need to raise additional skin flaps.
 Quadriceps Snip
Quadriceps Snip
If inadequate exposure has been afforded by the medial parapatellar arthrotomy and a complete intra-articular release, a quadriceps snip often provides enough additional exposure to complete the procedure safely.
The snip is made at the apex of the arthrotomy, obliquely across the quadriceps tendon at a 45-degree angle in line with the fibers of the vastus lateralis (TECH FIG 2).
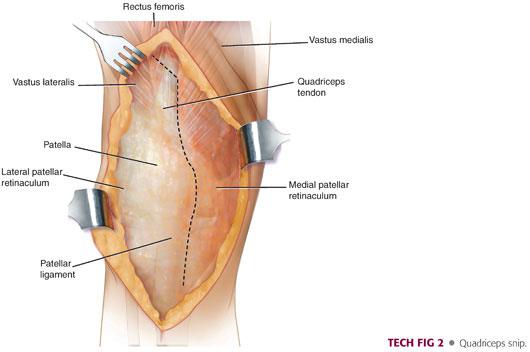
At the end of the procedure, the snip is closed side-to-side using nonabsorbable suture.
The postoperative therapy protocol is not altered if a quadriceps snip has been performed.
 Component Removal
Component Removal
The femoral and tibial components are then carefully removed as described in Chapter 44.
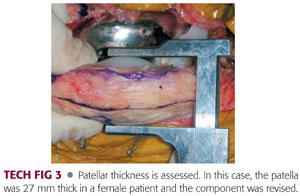
The patella then is assessed. Its thickness is determined (TECH FIG 3), and if the composite is considered to be too thick (ie, >25 mm for women and >30 mm for men) or in an otherwise suboptimal position (eg, lateralized), the component is removed.
If the component is to be retained, any osteophytes or unresurfaced sections of the native patella are removed.
 Recutting the Upper End of the Tibia and Performing a Posterior Release
Recutting the Upper End of the Tibia and Performing a Posterior Release
The proximal tibia is recut perpendicular to its mechanical axis with neutral slope. Either an intra- or extramedullary guide may be used. A neutral slope is recommended; rotation of the cut is not important at this point. The revision component often has an appropriate amount of slope built in (5 to 7 degrees) so that rotation in the optimal position can be set later.
A laminar spreader is then inserted both medially and laterally, and the scar tissue in the posterior aspect of the knee along with any remnant of the posterior cruciate ligament, if present, is removed completely to reestablish the flexion space and restore full extension (TECH FIG 4A).
At this point, ligamentous balance is assessed and appropriate releases are performed until the flexion gap is of equivalent size medially and laterally.
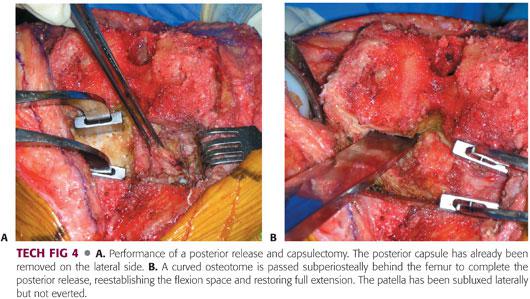
A curved osteotome is then used to release any remaining capsule from the posterior aspect of the femur and to clear any residual osteophytes retained at the time of the original TKA (TECH FIG 4B).
Given the tendency to elevate the joint line in revision TKA, a complete posterior capsular release is performed in all cases.
 Creating the Tibial Platform
Creating the Tibial Platform
The tibia is prepared first, as tibial height affects both the flexion and extension gaps.
The tibial component is sized to maximize coverage of the upper end of the tibia.
A stem typically is used to provide support for the revision component. Stems also assist with component alignment, particularly if a cementless diaphyseal engaging stem is selected. It is necessary to remember that the tibial shaft is offset posteromedially in relation to the center of the upper end of the tibia, and a stem that allows for offset is often required to optimize coverage of the upper end of the tibia (the stem is used to bring the component anterior and lateral in most cases).
The tibial trial component is then placed in the appropriate amount of external rotation; typically, the center of the component is aligned with the junction of the medial and middle thirds of the tibial tubercle (TECH FIG 5).

See Chapters 41 and 43 for additional details.
 Choosing the Femoral Trial Size and Augments
Choosing the Femoral Trial Size and Augments
Sizing of the femoral component can be difficult, but it is a critical portion of the procedure. If the original component is thought to have been too large, a smaller trial component is selected; however, in some cases, a larger femoral component will be needed to balance the flexion gap.
The surgeon must keep in mind that although it is desirable to leave the patient’s knee somewhat loose in flexion in cases of stiffness, this does risk flexion instability. Consideration should be given to using a more constrained insert in cases of revision TKA for stiffness.
The knee is initially trialed with a long intramedullary stem to assist with determining appropriate valgus alignment; a shorter stem can be substituted later if desired. Stems are used routinely, both to support the revision component and to assist with alignment.
The initial augments typically used include a posterolateral augment to encourage appropriate external rotation of the revision component and distal augments placed both medially and laterally to distalize the femoral component in response to the tendency of revision TKA to elevate the joint line.
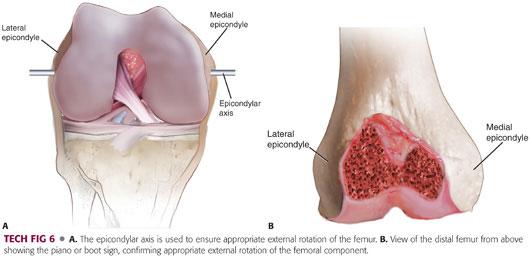
Appropriate external rotation of the femoral component is checked using the epicondylar axis of the femur (TECH FIG 6A). The surgeon also can check to make sure that a “piano” or “boot” sign is present when the cut surface of the femur is viewed from above (TECH FIG 6B). This sign indicates that the cut on the lateral side is deeper than that on the medial side, confirming appropriate external rotation of the femoral cut.
 Trialing and Closure
Trialing and Closure
The knee is now trialed with varying thicknesses of polyethylene liners to ensure
Full extension of the knee (TECH FIG 7A)
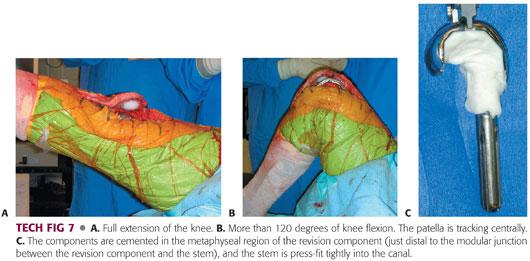
Adequate flexion of the knee (TECH FIG 7B). A good predictor of postoperative flexion is that achieved at the time of surgery with the knee flexed against gravity.
Adequate varus–valgus stability
Good patellar tracking. If patellar tracking is not acceptable, the rotation of the femoral and tibial components must be carefully assessed and changed if necessary until the patella tracks well.
Restoration of the joint line to within 1 cm of its normal position. The easiest way to assess the joint line is to compare the superior pole of the patella to the superior flange of the revision femoral component with the knee fully extended.
Various combinations of augments and polyethylene liners should be tried until the optimal combination is found; this may take a considerable amount of time to achieve.
The revision components are now assembled on the field. The stems can be either firmly press-fit into the diaphysis, with cement placed only around the metaphyseal segment of the component (TECH FIG 7C), or fully cemented, depending on the surgeon’s preference. Antibiotic-loaded cement is recommended, given the higher risk of infection in the setting of revision TKA.
The knee is closed in at least 90 degrees of flexion because this has been shown to increase final flexion. Following closure of the arthrotomy, ROM and patellar tracking are carefully assessed once again.
PEARLS AND PITFALLS | |
Indications |
|
| |
Pain management |
|
| |
Preoperative planning |
|
Perioperative evaluation for sepsis |
|
Retention of components |
|
| |
Patellar tendon avulsion |
|
| |










POSTOPERATIVE CARE
 Perioperative care must be monitored closely in conjunction with a pain management specialist and a physical therapist.
Perioperative care must be monitored closely in conjunction with a pain management specialist and a physical therapist.
 Patients are placed on a continuous passive motion (CPM) machine starting at 0 to 90 degrees in the recovery room, advancing the setting as tolerated. CPM is used for 4 to 6 hours per day and patients must understand that it is an adjunct to, not a substitute for, active and passive ROM exercises.
Patients are placed on a continuous passive motion (CPM) machine starting at 0 to 90 degrees in the recovery room, advancing the setting as tolerated. CPM is used for 4 to 6 hours per day and patients must understand that it is an adjunct to, not a substitute for, active and passive ROM exercises.
 The indwelling epidural catheter is continued for up to 6 weeks. The patient is seen by the surgeon and the pain management specialist weekly for the first 6 weeks to monitor progress.
The indwelling epidural catheter is continued for up to 6 weeks. The patient is seen by the surgeon and the pain management specialist weekly for the first 6 weeks to monitor progress.
 Patients are engaged in an aggressive physical therapy program emphasizing ROM, gait training, and strengthening.
Patients are engaged in an aggressive physical therapy program emphasizing ROM, gait training, and strengthening.
 If the patient has not achieved 90 degrees of flexion by 6 weeks, MUA is performed.
If the patient has not achieved 90 degrees of flexion by 6 weeks, MUA is performed.
OUTCOMES
 Table 1 summarizes the results of arthroscopic release, open arthrolysis, and revision TKA for the treatment of stiffness.
Table 1 summarizes the results of arthroscopic release, open arthrolysis, and revision TKA for the treatment of stiffness.
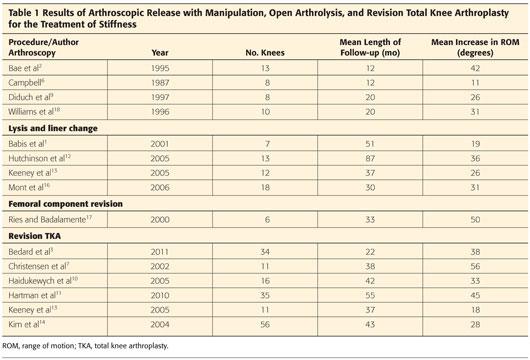
 Most of the literature suggests that revision for stiffness is associated with improvements in ROM, pain, and function, but that these gains are modest and, in a certain percentage of patients, stiffness will recur. Our own experience with a cohort of 35 patients showed that although 75% of patients had an improvement of at least 30 degrees of motion, the complication rate was high; nearly 50% of patients required some additional intervention to achieve that ROM.
Most of the literature suggests that revision for stiffness is associated with improvements in ROM, pain, and function, but that these gains are modest and, in a certain percentage of patients, stiffness will recur. Our own experience with a cohort of 35 patients showed that although 75% of patients had an improvement of at least 30 degrees of motion, the complication rate was high; nearly 50% of patients required some additional intervention to achieve that ROM.
 An arthroscopic release seems most appropriate for select patients with well-fixed, appropriately positioned and rotated components.
An arthroscopic release seems most appropriate for select patients with well-fixed, appropriately positioned and rotated components.
 Flexion contractures are particularly difficult to correct.
Flexion contractures are particularly difficult to correct.
COMPLICATIONS
 Recurrent stiffness
Recurrent stiffness
 Extensor mechanism disruption (particularly patellar tendon avulsion)
Extensor mechanism disruption (particularly patellar tendon avulsion)
 Infection
Infection
 Instability
Instability
 Neurovascular injury
Neurovascular injury
 Deep venous thrombosis
Deep venous thrombosis
REFERENCES
1. Babis GC, Trousdale RT, Pagnano MW, et al. Poor outcomes of isolated tibial insert exchange and arthrolysis for the management of stiffness following total knee arthroplasty. J Bone Joint Surg Am 2001;83:1534–1536.
2. Bae DK, Lee HK, Cho JH. Arthroscopy of symptomatic total knee replacements. Arthroscopy 1995;11:664–671.
3. Bedard M, Vince KG, Redfern J, et al. Internal rotation of the tibial component is frequent in stiff total knee arthroplasty. Clin Orthop Relat Res 2011;469:2346–2355.
4. Berger RA, Crossett LS, Jacobs JJ, et al. Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res 1998;356:144–153.
5. Bong MR, Di Cesare PE. Stiffness after total knee arthroplasty. J Am Acad Orthop Surg 2004;12:164–171.
6. Campbell ED Jr. Arthroscopy in total knee replacements. Arthroscopy 1987;3:31–35.
7. Christensen CP, Crawford JJ, Olin MD, et al. Revision of the stiff total knee arthroplasty. J Arthroplasty 2002;17:409–415.
8. Della Valle C, Parvizi J, Bauer T, et al. American Academy of Orthopaedic Surgeons clinical practice guideline on the diagnosis of the periprosthetic joint infection. J Bone Joint Surg Am 2011;90: 1355–1357.
9. Diduch DR, Scuderi GR, Scott WN, et al. The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166–171.
10. Haidukewych GJ, Jacofsky DJ, Pagnano MW, et al. Functional results after revision of well-fixed components for stiffness after primary total knee arthroplasty. J Arthroplasty 2005;20:133–138.
11. Hartman CW, Ting NT, Moric M, et al. Revision total knee arthroplasty for stiffness. J Arthroplasty 2010;25(6 suppl):62–66.
12. Hutchinson JR, Parish EN, Cross MJ. Results of open arthrolysis for the treatment of stiffness after total knee replacement. J Bone Joint Surg Br 2005;87:1357–1360.
13. Keeney JA, Clohisy JC, Curry M, et al. Revision total knee arthroplasty for restricted motion. Clin Orthop Relat Res 2005;440: 135–140.
14. Kim J, Nelson CL, Lotke PA. Stiffness after total knee arthroplasty: prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479–1484.
15. Laubenthal KN, Smidt GL, Kettelkamp DB. A quantitative analysis of knee motion during activities of daily living. Phys Ther 1972:52: 34–43.
16. Mont MA, Seyler TM, Marulanda GA, et al. Surgical treatment and customized rehabilitation for stiff knee arthroplasties. Clin Orthop Relat Res 2006;446:193–200.
17. Ries MD, Badalamente M. Arthrofibrosis after total knee arthroplasty. Clin Orthop Relat Res 2000;380:177–183.
18. Williams RJ III, Westrich GH, Siegel J, et al. Arthroscopic release of the posterior cruciate ligament for stiff total knee arthroplasty. Clin Orthop Relat Res 1996;185–191.
< div class='tao-gold-member'>



