Tongue-Lip Adhesion/Floor of Mouth Muscle Release for Pierre Robin Sequence
Chad A. Purnell
Arun K. Gosain
DEFINITION
Pierre Robin sequence (PRS) is a clinical triad of glossoptosis, retrognathia, and airway obstruction.
Cleft palate is present in approximately 50% of cases.
PRS is associated with an identified syndrome in 30% to 60% of cases.1
The most common syndromes associated with PRS are Stickler syndrome (11%-20%) and 22q11.2 deletion (velocardiofacial) syndrome (11%).2
ANATOMY
The tongue in PRS is posteriorly displaced due to retrognathia. This results in an airway obstruction at the tongue base (FIG 1).
Airway obstruction may also result from lesions lower than the tongue, such as laryngomalacia. Synchronous airway lesions are present in up to 28% of patients.3
Cleft palate may be U- or V-shaped; a U-shaped palatal cleft is classically associated with PRS.
PATHOGENESIS
Pathogenesis of PRS is incompletely understood and likely multifactorial.
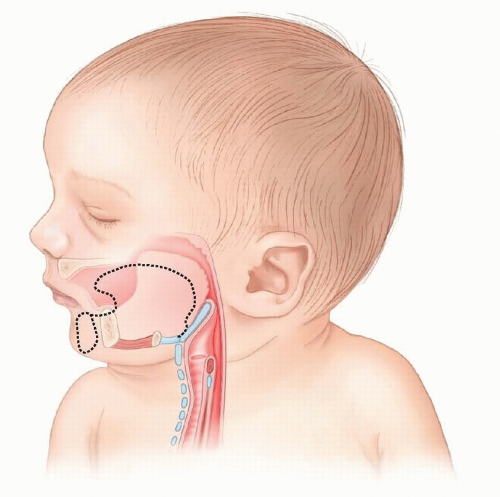 FIG 1 • Micrognathia results in a more posterior position of the mandible and tongue in PRS (solid lines) compared to a normal patient (dotted lines). |
NATURAL HISTORY
PRS occurs on a spectrum that ranges from mild asymptomatic hypoplasia to critical airway obstruction requiring emergent endotracheal intubation at birth.
In more severe phenotypes, PRS is often associated with feeding issues such as gastroesophageal reflux, failure to thrive, and abnormal oroesophageal motility.6,7
PATIENT HISTORY AND PHYSICAL FINDINGS
A full birth history and physical examination should be performed. A key point of examination should be documenting the maxillomandibular discrepancy with the child upright and the mandible closed.
A careful examination for syndromic features should include hearing and ocular exam to evaluate for Stickler syndrome.10
Evaluation and treatment of any patient with PRS should be performed by a multidisciplinary team, which includes craniofacial surgery, otolaryngology, speech and feeding therapy, critical care/anesthesiology, and genetics.
IMAGING
If the child is not intubated, a polysomnogram should be performed, including a portion with a nasopharyngeal airway in place in order to determine whether there is ongoing sleep apnea if upper airway obstruction is removed.
Fiberoptic nasendoscopy is performed to evaluate whether the airway obstruction is isolated to the tongue base or whether there are additional sources of supraglottic airway obstruction, including laryngomalacia.
Prior to any surgical intervention, bronchoscopy should be performed to evaluate for subglottic synchronous airway lesions.
NONOPERATIVE MANAGEMENT
The majority of patients can be treated nonoperatively.
Initial airway management is prone positioning to displace the mandible anteriorly.
Supplemental oxygen may be added as well.
A nasopharyngeal airway should be placed if desaturations continue. This airway has been utilized successfully as end-treatment at home by several centers.11
If a nasopharyngeal airway does not resolve airway obstruction, emergent endotracheal intubation is indicated.
SURGICAL MANAGEMENT
Preoperative Planning
Prior to any surgical treatment, bronchoscopy should be performed. In the presence of significant subglottic obstruction, tracheostomy is likely the only treatment option.
Prior to performing a tongue-lip adhesion, a GILLS score should be calculated. One point is given for each of the following: gastroesophageal reflux, intubation preoperatively, late operation (greater than 2 weeks of age), low birth weight (less than 2500 g), and syndromic diagnosis. A score of 3 or more is predictive of failure of tongue-lip adhesion, and another option such as mandibular distraction osteogenesis or tracheostomy should be considered.14,15
Positioning
The procedure is performed supine.
Endotracheal intubation may be nasotracheal or orotracheal, with the tube taped to the side out of the operative field.
Approach
Soft tissue procedures for PRS include tongue-lip adhesion, subperiosteal release of the floor of mouth, or both procedures performed concomitantly.16,17
Subperiosteal release of the floor of mouth is an ideal addition to tongue-lip adhesion if the patient has a fixed, immobile tongue (ankyloglossia) and a tongue-based airway obstruction. This procedure is also performed in isolation for airway obstruction at some centers.
Mandibular distraction osteogenesis is a skeletal technique to treat mandibular hypoplasia that may have more repeatable resolution of airway obstruction in a broader range of patients with PRS, with potentially higher complication rates.18,19,20Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree