Fig. 9.1
Facial subcomponents used to derive our classification for the chin shape in the frontal view.
Lower central border (blue line), lateral borders (yellow dotted line), central–lateral junction (arrow), geniomandibular junction (dotted arrow), lower facial line (green dotted line), and soft tissue overlying the chin (red dotted circle)

Fig. 9.2
Classification of the chin shape in the frontal view.
From left to right: round chin, broad chin, blunt chin, angular chin, trapezoid chin, triangular chin, pointed chin, and pear-shaped chin types
Classification of Chin
- 1.
A round chin has a smooth, curved lower chin border without a definite central–lateral or geniomandibular junction, and the overall contour of the lower facial line is circular. Thus, the chin appears to be part of a circle.
- 2.
A broad chin exhibits a curved to flat lower central border without a definite central–lateral junction and with a convex geniomandibular junction. This is the vertically elongated variation of the round type, giving a U-shaped appearance to the lower face.
- 3.
A blunt chin exhibits a curved lower chin border and a smooth and clear central–lateral junction. Because this type has a developed chin pad, it looks blunt in the frontal view.
- 4.
An angular chin shows a characteristic linear, wide lower central border with a less developed chin pad. It also exhibits a sharp, acute central–lateral junction, an angular geniomandibular junction, and a developed mandibular angle; consequently, the lower facial line looks like part of an octagon.
- 5.
A trapezoid chin exhibits a curved, narrow lower central border, smooth central–lateral junction, and straight geniomandibular junction. The difference from a triangular chin is the presence of a horizontal component in the lower central border.
- 6.
A triangular chin is defined by a negligible lower central border with an indefinite central–lateral junction and a straight geniomandibular junction, thus appearing as an inverted triangle.
- 7.
A pointed chin exhibits a narrower bigonial width and/or a vertically more elongated chin height compared with the triangular type. Therefore, the width–height ratio of the lower third of the face is smaller than that with a triangular chin.
- 8.
A pear-shaped chin is defined by a concave geniomandibular junction, thus looking like a pear. For a better understanding, typical clinical photographs of each type are shown in Fig. 9.3
Fig. 9.3
Typical clinical photographs of representative cases with each chin type as per our classification
Patient Assessment
In ID hospital, this classification is used when assessing each patient’s chin shape and their preference about the chin shape. Our investigation results indicated a discrepancy between the actual prevalence and the patient preference; patients prefer narrower chin shape (triangular, trapezoid), while the actual shapes in Koreans and Asians comprise broad, round, and angular types. Therefore surgeon should customize the correction surgery for the frontal chin shape according to the actual shape and patient preference.
The width of chin is the most important factor to determine the amount of narrowing. When surgeons consult with patient, careful assessment of the present width of chin and desired width of chin is critical. The amount of narrowing central segment ranges from 4 to 12 mm in most cases.
The height of chin is also important because the width–height ratio eventually determine the impression of slender. Ideal height of chin is considered as double the height of upper lip, in other words, the distance from the subnasale to the stomion. If the height is too long or too short compared with the ideal one, vertical reduction or lengthening should be performed simultaneously with narrowing genioplasty (Chaps. 10 and 11).
Then, asymmetry should be considered. Significant asymmetry of chin can be corrected by midline shift and asymmetric central segment resection (Fig. 9.4).
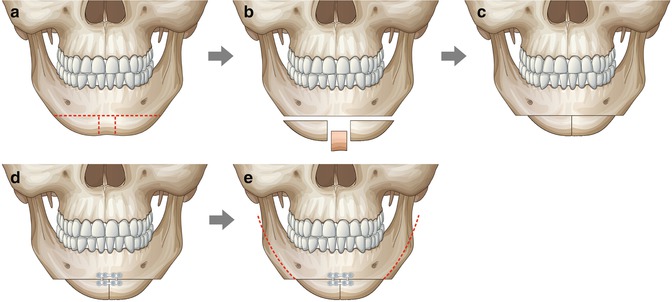
Fig. 9.4
Illustrations of surgical procedures of the V-line surgery. (a) Avoiding the inferior alveolar canal and mental foramen, one horizontal and two vertical osteotomies were performed. (b) The central strip was removed. (c) Two distal segments were approximate centrally. (d) Fixation with plate and screws was performed. In order to prevent possible loosening and rotation, at least two screws were used to fix each distal segment. (e) Mandible contouring starts from the anterior step to the posterior ramus according to the planning. It is important to preserve inferior alveolar canal
Finally profile view of chin should be assessed as introduced in Chap. 10. If the position of the pogonion is backward or forward compared to the ideal one, advancement or setback of the two distal segments is required.
Surgical Techniques
- 1.
The approach to the mid-symphyseal area was accomplished with a conventional intraoral vestibular incision and subperiosteal dissection. Soft tissue attachment of the chin was maintained to produce a maximum narrowing effect and maintain the blood flow to bony segments.
- 2.
Horizontal osteotomy and two vertical osteotomies were designed as shown in Fig. 9.2. The amount of resection in the central segment was determined preoperatively, depending on the width of chin and the patient’s desire. In proportion to the shape of the chin, the shape of the central segment to be resected can be altered from a triangle to a trapezoid or rectangle.
- 3.
After osteotomy was completed, the muscular attachment was stripped off, and the central segment was removed. Two segments were approximated centrally and fixed with plates and screws.
- 4.
Advancement or setback of the two segments is also possible if correction of the profile is required. In case of asymmetric chin, midline shift and asymmetric central segment resection are required.
- 5.
After fixation of distal segments, the bony edge of the lateral and proximal mandible remains. This is the different feature from conventional angle resection. So, the surgeon should check the exact amount of the bony step between the lateral edge of distal segment and proximal mandible by direct vision and manual palpation.
- 6.
Then, mandible contouring is started from the nearest point between inferior alveolar nerve canal and lower border of the mandible. To avoid damage to the inferior alveolar nerve, guarded saw is used at this point at least 2–3 mm apart from the lower border of inferior alveolar canal.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree