Fig. 27.1
Superficial anatomy of the facial mimetic muscles involved in the aging process

Fig. 27.2
(Arrow) Vertical vector of descent of the malar fat pad typical of the aging process causing accentuation of the nasolabial fold

Fig. 27.3
Aging process also involves vertical downward migration of superficial mimetic muscles

Fig. 27.4
(Arrow) Malar fat pad repositioned vertically to the original anatomy

Fig. 27.5
Postoperatively the facial anatomy is restored to a more youthful position
27.4 The Stem Cell-Enhanced Regenerative Facelift
This is a combination of procedures: each of them could be used singularly or together depending on the preoperative assessment. Namely, it consists of four technical gestures
1.
Facial hydrofilling and wide supramimetic muscle undermining of skin flap
2.
Orbiculo–zygomaticus–levator labii–platysma pexy
3.
Submuscular and subperiosteal placement of stem cell-enriched graft
4.
Vest over pants tension-free skin closure with triangular tragus flap closure
27.5 Technique
27.5.1 Facial Hydrofilling and Wide Supramimetic Muscle Undermining of Skin Flap
Facial hydrofilling consists of filling the superficial dissection plane with a solution similar to the one used for liposuction. It is not a tumescent technique because, in the author’s opinion, if too much fluid is used, it would be detrimental for evaluating the tension of the final skin redraping maneuver and it would compromise long-term results. Approximately 100–120 mL of fluid is used. The injection is done with a blunt cannula to avoid excessive bruising. The hydrofilling allows developing a thicker skin flap and makes the dissection technically easier to perform. Furthermore, along with the use of electrocautery, it minimizes bruising, hematoma, and risks of flap viability issues.
The patient is seen in the preoperative area, and the incisions are marked with the patient sitting up. The cheeks, chin, and angle of the mandible implant sizers are used to delineate the areas of volume enhancing. A hairline incision is planned in the temporal area, a post-tragal incision in the preauricular area, and then the incision is carried into the hairline in the mastoid area. Only in case of heavy necks or really redundant skin, the postauricular occipital incision is made in the hairline.
General endotracheal anesthesia is induced. The first step consists of injecting the incisions with local anesthetic (Xylocaine 1 % with epinephrine 1:100,000), and then the facial hydrofilling is performed. The entire face and neck is injected with a solution consisting of 1 liter of normal saline, 50 mL of plain Xylocaine 1 %, and 1 mL of epinephrine 1:1,000 with a blunt cannula. Approximately 100–120 mL of solution is injected each site.
After the skin is incised, the approach consists of developing a tick flap right off the SMAS-parotid fascia and the mimetic muscles. The dissection is performed with electrocautery and a Colorado needle point. 2.5 loops are used. External and internal countertraction are critical, and it is performed by the assistant over the external skin distant to the area of dissection and internally by the surgeon himself with a forceps, so a clear-cut plane of dissection is visualized. The electrocautery dissection (along with the hydrofilling) allows to maintain a bloodless surgical field so critical for recognizing anatomical landmarks (Fig. 27.6). The dissection starts postauricular in the mastoid area. Care is taken to leave as much subcutaneous fat as possible attached on the skin flap. The dissection is carried posteriorly widely. The width is critical posteriorly to be able to improve the skin redundancy of the neck and create a long-lasting result.
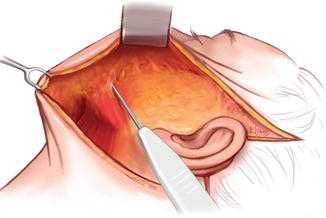
Fig. 27.6
Supramimetic facial muscles undermining of skin flap with electrocautery; Note the thickness of the skin flap where most of the subcutaneous tissue is left on the flap itself which allows a better blood supply. Also note the undermining is very wide
Too often the lateral neck dissection is underdone and the central part overdone either through excessive liposuction or medial platysma placation. The lateral edge of platysma is visualized, and careful dissection with electrocautery is performed over the platysma down toward the clavicle to reach the base of the neck. It is the author’s opinion that in thin and regular size neck the central plication of the neck should be avoided. The platysma muscles are normally separated in the midline in young patients, and that does not seem to have any role in causing any aging issues: the goal should be to reinstate the normal anatomy not to change it. Only in thick and short necks where the gain of creating a sharper contour is more critical that the risk of irregularities is a midline plication along with liposuction is performed.
The attention is then turned to the elevation of the skin flap preauricularly. The dissection proceeds superiorly to visualize the orbicularis oculi muscle and proceeds inferiorly and medially to skeletonize the zygomaticus mayor and minor muscle and the levator labii. The plane of dissection is right over the muscles and extends over the platysma in a supra platysma fashion well described by Hoefflin. The elevation continues over the depressor anguli oris, depressor labii inferioris, and mentalis. This dissection allows not only the division of all the restraining ligaments but it skeletonizes the superficial facial muscles so their edges are clearly delineated. The key is elevating a really wide and thick skin flap (Fig. 27.7).

Fig. 27.7
Blue area is the area of skin flap undermining. Only by wide undermining it is possible to move the facial tissue in a “true” vertical direction
27.6 The Orbicularis Oculi–Zygomaticus–Levator Labii–Platysma Pexy
This technique can be used by itself or, more commonly by the author, in combination with other techniques of tridimensional facial augmentation. Once hemostasis is obtained, then the mimetic muscles pexy is planned. By only elevating a very wide skin flap, the mimetic muscle plication can be executed in a vertical vector (Fig. 27.8). Most of the SMAS techniques limit the skin undermining in the cheek area for anatomical reasons. A wider undermining would interfere with the SMAS attachment and the SMAS flap itself would loose its insertion in the nasolabial fold. By definition in any SMAS technique the plication is limited to the degree of the undermining and it is generally more lateral then medial therefore a true vertical vector of tissue repositioning is not applicable. Convinced of some benefits of the SMAS, but aware of some of the short comes, the orbiculo–zygomaticus–levator labii–platysma pexy has been developed in the effort to reposition more directly and more in a vertical vector some of the facial musculature affected by gravitational forces (Fig. 27.9). This technique can be used by itself or, more commonly by the author, in combination with other techniques of tri-dimensional facial augmentation.
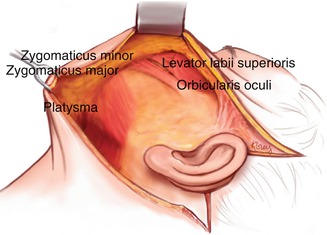

Fig. 27.8
Extent of dissection of the skin flap and skeletonization of mimetic muscles is the key to reposition the tissues in a vertical direction
Fig. 27.9
(Arrows) Vertical vectors of repositioning of facial musculature. Red line depicts line of levator labii–orbicularis–zygomaticus–platysma pexy
Related posts:
 Stem Cell Applications: An Overview
Stem Cell Applications: An Overview
 The Adipose Organ: Morphological Perspectives of Adipose Tissues
The Adipose Organ: Morphological Perspectives of Adipose Tissues
 The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
The Role of Adipose Tissue-Derived Stem Cells and of Angiogenesis
 Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
Advantages of the Transplantation of Fat in Plastic and Reconstructive Surgery
 Hand Rejuvenation with Stem Cell Fat Transfer
Hand Rejuvenation with Stem Cell Fat Transfer
 Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stem Cell Fat Transfer for Mastoplasty Using VASER™ Ultrasound and Office-Devised Stem Cell
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


