Fig. 17.1
Coronal scalp incision design for reduction malarplasty
Surgical Technique
The procedure is performed under general anesthesia with endotracheal intubation. Fiber-optic headlight comes in very handy when illumination of the malar area under the coronal flap is needed. The incision is made after local anesthetic solution (0.5% lidocaine with 1:300,000) epinephrine is infiltrated. An incision beveled parallel to the hair shafts is made down to the pericranium, and subgaleal dissection is performed downward to the supraorbital rims. Once reaching the supraorbital rims, dissection is changed to the subperiosteal plane to expose the malar body, zygomatic arch, lateral orbital wall, and anterolateral maxillary wall. The temporalis fascia insertion site and masseteric attachments to the malar bone are left intact except at the sites of osteotomy. The reason for this is preservation of pulling forces acting on the zygoma and bloody supply.
Medial and lateral malar osteotomies are made to mobilize the malar complex. Both osteotomies are performed with a reciprocating saw, while soft tissue is protected with retractors. The medial osteotomy line starts at the maxillary notch, which is located 5–8 mm medial to the inferior end of zygomaticomaxillary suture and extends straight upward, ending near the frontozygomatic suture while preserving the lateral orbital rim. The maxillary sinus may be opened during medial osteotomy, but this has not produced significant complications such as infection, sinusitis, or bleeding, in our experience. Placing the medial osteotomy line too far laterally out of fear for damaging the orbital contents may lead to undercorrection and stepping deformity in the anterior cheek. As far as the blade of the saw is directed in the proper axis and direction, there is no risk of entering the orbital cavity. The lateral osteotomy line is drawn just anterior to the zygomatic tubercle. The zygomatic arch is cut obliquely from posterior to anterior (Fig. 17.2). Once the osteotomies are made, the malar complex is repositioned to the desired location and is stabilized with interosseous wires or miniplates and screws. There are two options with differing indications: transpositional malarplasty or in situ reduction osteoplasty.
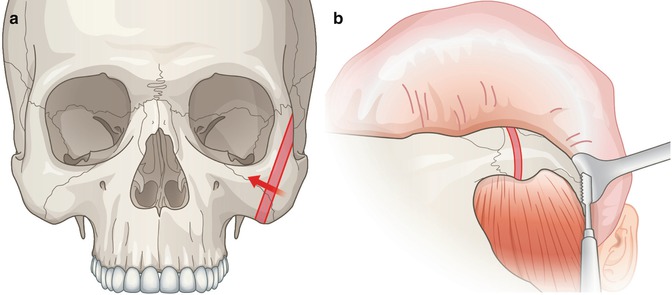
Fig. 17.2
Medial osteotomy (a) is made and a strip of bone is removed to reduce lateral prominence. Lateral osteotomy (b) is made after completing medial osteotomy
The transpositional malarplasty technique is employed for patients with asymmetric malar complexes, severe prominences, or descended zygomatic body complex. After osteotomy, the malar complex is completely released to mobilize for ideal position and reduced by ostectomy with sawing and marginal burring. This technique achieves the ideal repositioning of malar prominence by (1) adequate ostectomy and (2) three-dimensional transpositioning of the zygomatic complex for most attractive facial balance. After reduction, the malar complex should be secured with wires or miniplates.
The second method is termed in situ reduction osteoplasty. Indications are symmetric malar complexes, mild to moderate prominence, or zygomatic arch prominence. Medial osteotomy plane is designed to make the zygomatic complex slide posteromedially to reduce lateral excess. Next, the zygomatic arch is cut obliquely for bone Z-plasty. Finally, the malar complex is repositioned with the anterior segment of the zygomatic arch slid posteriorly and medially and is fixed in place with wires.
Bone dust is removed thoroughly by irrigation before wound closure. The galea is closed with interrupted Vicryl 4-0 sutures and the skin is closed with staples. Drains are not inserted. Compressive dressing is done with elastic net applied over the head.
Key Technical Points
- 1.
The coronal scalp incision line follows the frontal hair pattern and is drawn 8 cm posterior to the anterior hairline. In the temple area, the incision curves downward until reaching the junction of the superior helix of the ear with the temporal scalp.
- 2.
During dissection through the coronal approach, the temporalis fascia insertion site and masseteric attachments to the malar bone are left intact except at the sites of osteotomy, to preserve pulling forces acting on the zygoma and bloody supply.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree