Globe prominence (proptosis) may be caused by a variety of congenital or acquired conditions and poses unique challenges to aesthetic and reconstructive surgery. Once the underlying cause of proptosis is determined, a treatment plan consisting of surgical and medical procedures can be formed. Thyroid eye disease is the most common cause of proptosis and helps guide treatment options for proptosis. Although common eyelid and orbital procedures are used for proptosis correction, special care must be taken due to the unique difficulties of the distorted anatomy. Various surgical procedures and less invasive treatments can be combined to provide optimal aesthetic and functional results.
Key points
- •
Proptosis may be caused various congenital or acquired conditions, with thyroid eye disease being the most common acquired etiology.
- •
Untreated globe prominence can lead to a variety of complications due to the potential for diminished mechanical function of the eyelid.
- •
Globe prominence and its associated features may be managed conservatively with injectable fillers and/or botulinum toxin type A or surgically via orbital decompression, blepharoplasties, and facial contouring procedures.
- •
Familiarity with eyelid and orbital anatomy and surgical treatment options is imperative in producing a good aesthetic and functional result.
Introduction
The prominent globe (proptosis) poses a unique set of challenges to the surgeon attempting aesthetic or reconstructive surgery. Physicians must pay special attention to avoid poor outcomes or worsening aesthetic appearance or causing ocular or visual disturbances. Patients are at risk for a variety of complications, due to potential diminished mechanical function of the eyelid, such as scleral show, lagophthalmos, strabismus, eyelid retraction, exposure keratopathy, and ulceration. ,
Globe prominence can be associated with a variety of congenital conditions, such as a shallow orbit, hypoplasia of the maxilla and zygoma, or craniofacial syndromes (Crouzon or Pfeiffer syndromes). , Additionally, a prominent globe may be seen with increased axial length of the globe, such as in moderate to high myopia. Most commonly, a prominent globe is due to an acquired disease state, such as thyroid eye disease (TED). ,
It is imperative that patients with prominent globes are diagnosed and managed before aesthetic interventions. For example, patients with TED can experience a variety of clinical manifestations that lead to changes in their facial anatomy. These manifestations can include eyelid swelling, eyelid retraction, proptosis, strabismus, brow fat expansion, preaponeurotic fat expansion, glabellar rhytids, and expansion of the soft tissues in the cheeks, buccal fat, and eyebrows. , Attempting to correct patients’ cosmetic concerns with subtractive upper and lower blepharoplasty without addressing the position of the globe or orbital rim results in suboptimal outcomes and has the potential to cause debilitating exposure symptoms, tearing, and unfavorable cosmetic results. , Due to these potential complications, it sometimes is necessary first to perform surgery aimed at altering globe position and orbit architecture before performing cosmetic periocular procedures.
This article reviews the various treatment options that should be considered when evaluating a patient with a prominent globe. Although TED is the primary etiology of globe prominence that this article focuses on, these treatment modalities can be utilized in treating any cause of a prominent globe. No matter the etiology, the underlying cause of a prominent globe should be identified and addressed as needed before cosmetic procedures are attempted.
Anatomic associations
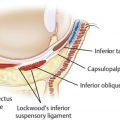
The normal position of the lower eyelid is maintained by a balance of tendons, ligaments, muscle, and orbital volume. The medial and lateral canthal tendons function as a sling to maintain the eyelid height and anatomic position along the undersurface of the globe. Ligaments keep the soft tissue of the eyelid and cheek attached the facial bones. Of primary concern to eyelid surgeons is the orbicularis muscle, which tonically contracts in a sphincteric fashion to maintain lower eyelid position. Finally, the fat and bone that maintain the orbital volume provide stability to the face and the lower eyelid. This delicate balance easily can be disrupted and lead to lower lid retraction, particularly in patients with globe prominence.
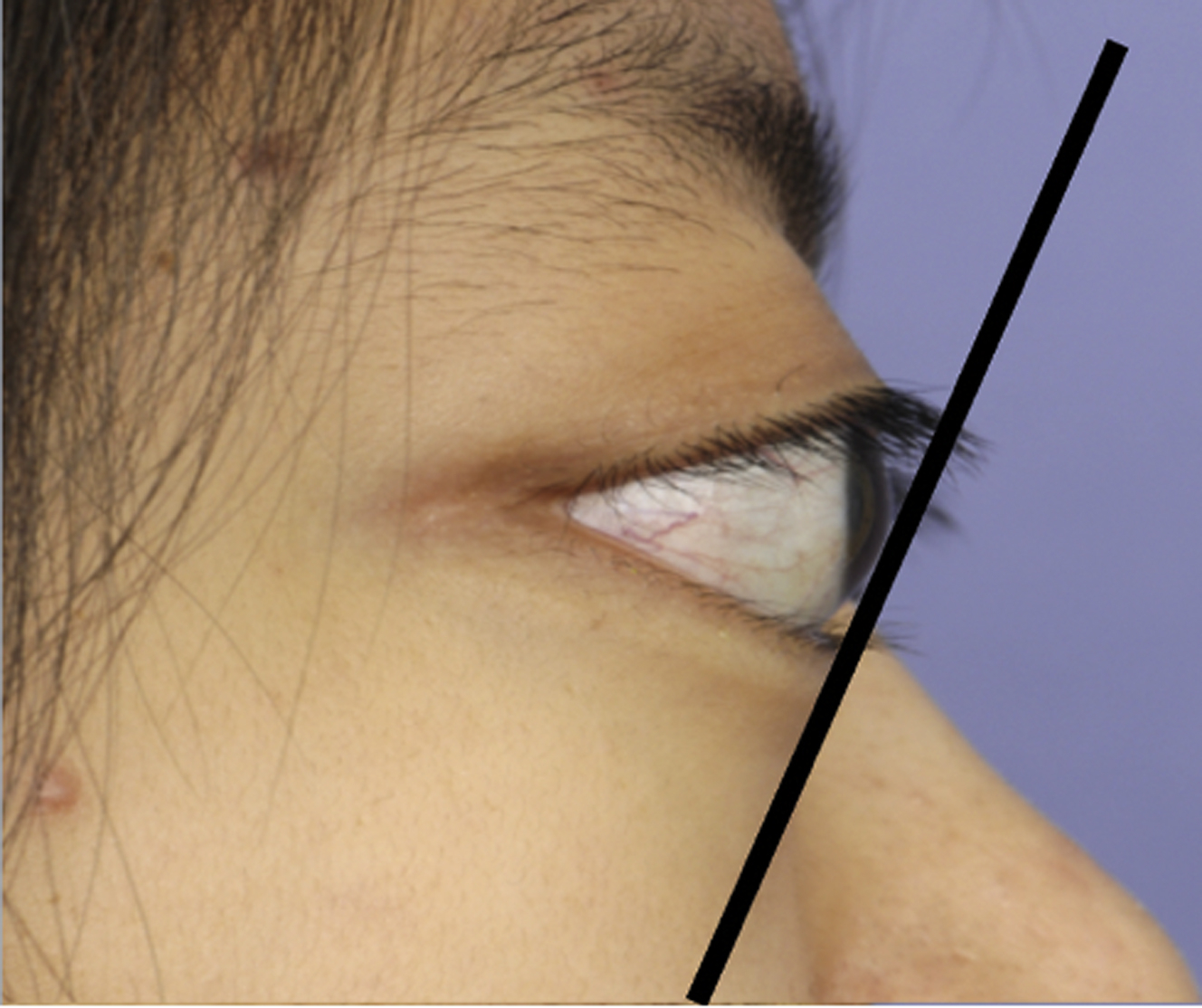
Globe prominence may be due to an increase in the volume of fat and/or ocular muscles, such as in TED, nonsyndromic exorbitism, midface hypoplasia, soft tissue or bony lesions, or a congenitally enlarged globe. , All these conditions create a negative vector eyelid, in which the cornea protrudes past the malar eminence. , , Patients with negative vector eyelids are at greater risk of experiencing lower lid malposition after aesthetic surgery due to the force exerted by the prominent globe on the lower eyelid, which forces the eyelid to support itself against the upward slope of the globe ( Fig. 1 ). , For example, when patients have globe prominence with a negative vector eyelid, special care must be taken in the canthal suspension of lower eyelid blepharoplasty in order to avoid bowstringing of the globe.
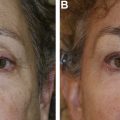
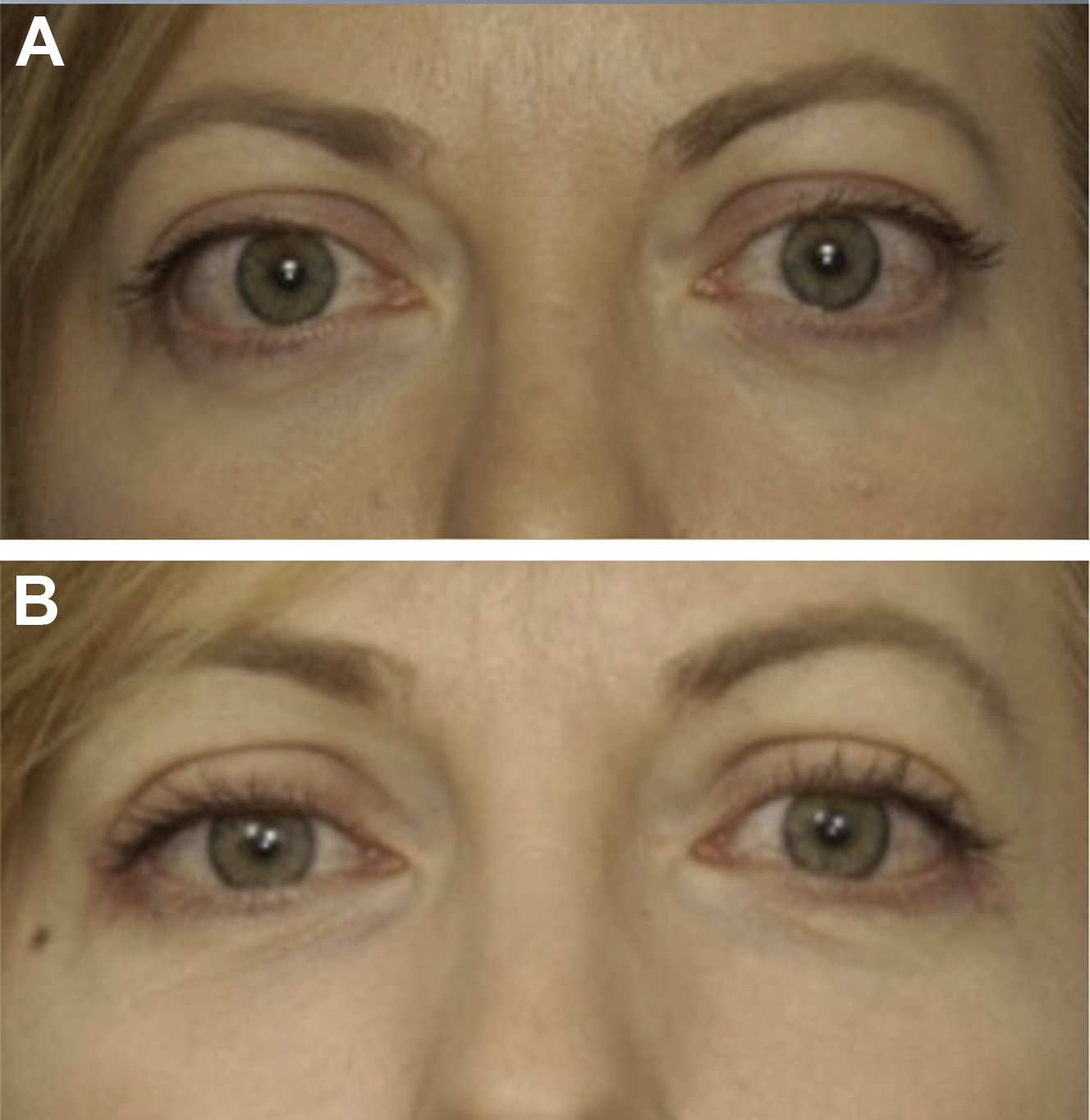
Patients with prominent globes, including those patients with TED, tend to have eyelid retraction, a high upper eyelid crease, increased periorbital volume/fat prolapse, and increased prominence of tear trough ( Fig. 2 ). Each of these physical findings requires recognition and thoughtful evaluation and surgical planning because patients with prominent eyes require more complex techniques to avoid unnecessary complications.

Surgical treatment options
Surgical treatment options for globe prominence and eyelid retraction have evolved over the years to become less invasive, produce better cosmetic results, and provide greater patient satisfaction. Because TED is the most frequent etiology of globe prominence or proptosis, we are using TED as an example to frame this discussion.
The traditional surgical management of non–vision-threatening TED included a 4-staged surgical approach of orbital decompression, eye muscle surgery, correction of eyelid malposition, and blepharoplasty. This approach was believed to increase predictability because each step would affect the planning of the subsequent procedures, ultimately producing the best result in the fewest procedures. The multistaged approach, however, has disadvantages, such as a lengthy patient time commitment due to the need for a healing interval between surgeries, increased patient cost, high patient anxiety, and added incisions and healing leading, to the formation of more scar tissue, all of which can factor into decreased patient satisfaction. Recently, studies have shown that orbital decompression surgery produces predictable changes in eyelid position and contour. Furthermore, a single-staged facial reconstruction, including bilateral orbital, aesthetic eyelid, and facial surgery, produces safe, efficacious, and predictable aesthetic results that are comparable to those from a multistaged approach with fewer disadvantages and less downtime ( Figs. 3 and 4 ). These studies clearly demonstrate how globe prominence affects the eyelid contour and relative height ( Fig. 5 ).


The authors recommend a customized approach to aesthetic reconstructive surgery based on an individual’s facial characteristics and changes that have occurred due to eye prominence. There is great individual variability in the facial anatomy, including periorbital bone projection and soft tissue expansion in the cheeks, buccal fat, and eyebrow. It is imperative that the surgeon considers the patient’s inherent facial structure as well as the changes due to TED, rather than limiting the surgical goal to globe positioning, when planning surgery. Furthermore, the surgeon should evaluate each patient thoroughly and discuss the orbital and periorbital changes within the context of their facial morphology and aging process so that realistic surgical plans and goals that reduce the effects of TED can be established. discuss the orbital and periorbital changes within the context of the facial morphology and aging process so that realistic surgical plans and goals. With TED, the surgeon should stress that the goal of surgery is to improve their function and appearance as closely as possible to their predisease state, but that complete rehabilitation not always is possible. Predisease photographs help the surgeon and patient develop realistic expectations for the surgery.
Orbital decompression
Although orbital decompression initially was performed only in vision-threatening cases due to optic neuropathy or uncontrollable ocular exposure, improved and minimally invasive techniques have led to expanded indications for purely cosmetic purposes. Orbital decompression surgery should be customized to each patient, taking into account the type and magnitude of decompression necessary, all of which likely reduce the need for additional eyelid or periorbital procedures. It is imperative that the physician considers each patient’s clinical characteristics, such as compressive optic neuropathy, eyelid retraction, fat versus muscle predominant disease, and nonaxial globe displacement, when surgical planning. ,
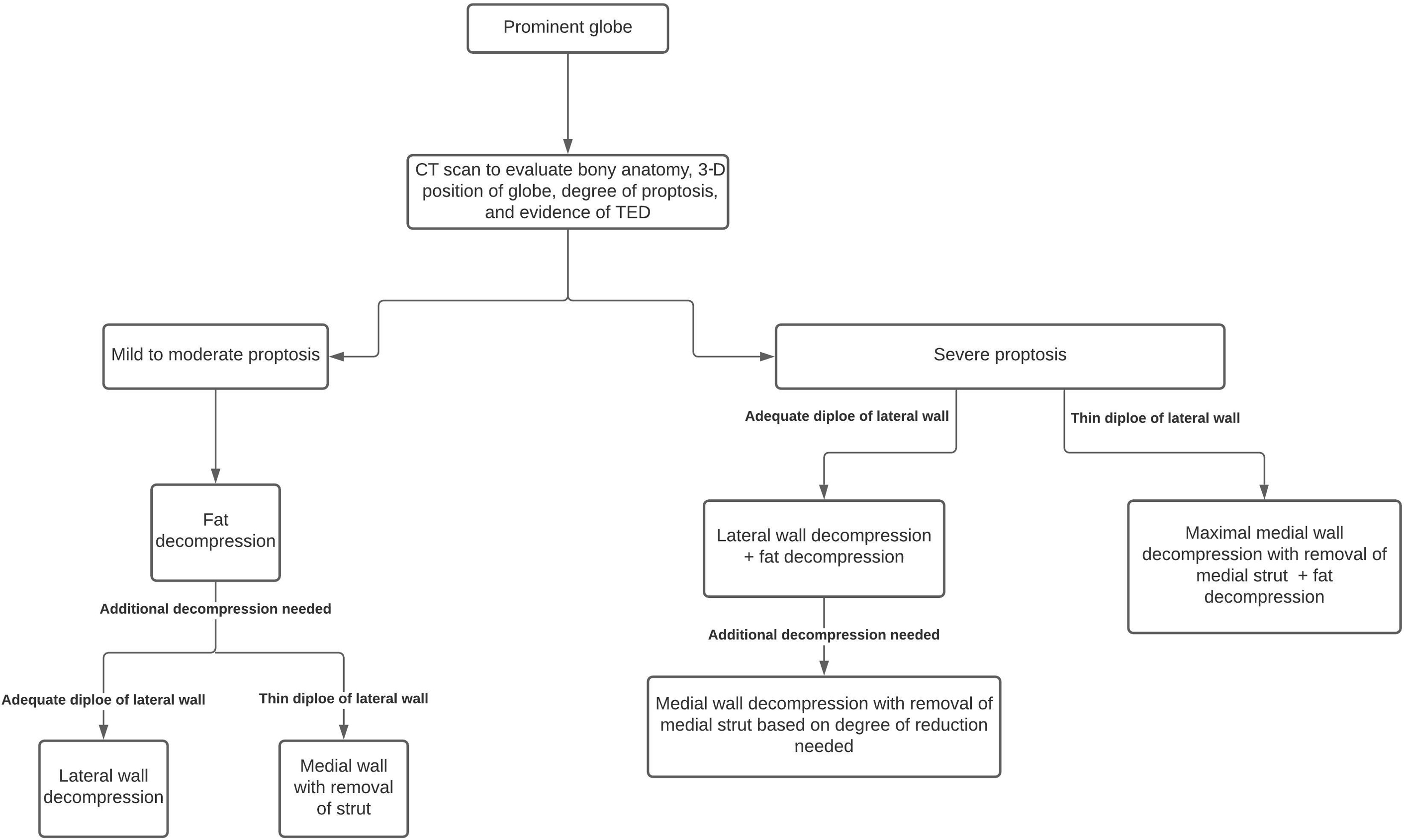
Planning for aesthetic reconstruction for patients with prominent globes begins with an evaluation of the 3-dimensional (3-D) globe position, which helps guide the type and magnitude of potential orbital decompression ( Fig. 6 has a flow diagram). It is important that preoperative computed tomography (CT) scan be performed so that the bony anatomy can be assessed, including the diploe of the lateral wall, to plan the amount of bone decompression. The most common anatomic targets for decompression are the deep lateral orbital wall, medial wall, and orbital floor. The authors prefer a deep lateral orbital decompression demarcated by decompression posterior to the course of the zygomaticotemporal nerve to achieve significant axial reduction from the zygomatic basin (inferolateral orbit adjacent to the inferior orbital fissure), superior lateral, and deep sphenoid ( Fig. 7 ). Orbital fat removal is the initial step in orbital decompression not only in fat predominant fat-predominate TED but also muscle-predominant and mixed disease. Fat decompression can be the initial step in the management of prominent eyes in patients without TED. Decompression in the region of the zygomatic basin can help reduce relative hyperglobus as well as improve the relationship of the lower eyelid and globe, reducing lower eyelid retraction in a highly predictable manner. This method potentially eliminates the need for lower eyelid retraction repair in mild to moderate TED and in cases of eyelid retraction without TED. The most severe cases of TED may require lower eyelid retraction repair, performed via recession of the lower eyelid retractors or placement of hard palate grafts, although in the authors’ practice these circumstances are rare. Further reduction in axial proptosis also may be achieved as needed with fat decompression, which is especially effective in fat predominant disease. , , redundant.