Key points
- •
For the last 10 years, vertical reduction mammaplasties have become a modern trend in breast reductions. Some surgeons, however, are reluctant to adopt them because they consider that the procedure is neither easy to learn nor is it easy to obtain a nice, shaped projected breast. Additionally, the results can not be observed at the end of the surgery. The circumvertical technique is easy to learn. The parenchyma removal and its remodeling is the same as in the w-pattern techniques and a round-shaped breast is observed at the end of the surgery.
- •
In the circumvertical technique, the skin is de-epithelialized as in circumareolar plus vertical techniques. The inferior half of the breast skin is undermined and separated from the pectoralis fascia.
- •
The parenchyma removal follows the w-pattern. Pillars are firmly sutured in two to three layers or imbricated to build a round-conic projected breast whose inferior edge is sutured to the pectoralis facia.
- •
The areola is transposed without any pedicle. The areola is sutured using the cinching running suture.
- •
At the end of the surgery a nice, round-shaped breast is observed with a harmonious distribution of the wrinkles around the areola. The vertical scar never crosses the submammary fold.
- •
Most of the inferior breast skin resected in the inverted T technique will retract in the circumvertical technique and will become part of the chest wall.
Patient selection
This technique is indicated when there is an acceptable volume of good skin quality, when the amount to be removed is less than 1000 g and when the areola elevation is no more than 10 cm. During the surgery I follow the penciled line and the estimation of the glandular removal I planned before surgery. This is especially important when there are asymmetries. As there is a great variety of breast hypertrophies, before surgery, I also plan from which part of the breast I have to remove more tissue and, when there are difficult asymmetries, I draw a draft of the future areas to be removed as a surgical guide.
Indications
I use the periareolar technique in minor hypertrophies. The circumvertical is a technique which should only be used in moderate or big hypertrophies but good results are not obtained in gigantomasties, where the vertical scar usually trespasses the submammary fold (SMF) or the vertical has to be transformed into an inverted T technique. When the patient has firm skin, the skin is marked and then resected in a conservative way, because during and after surgery, it will retract.
Operative technique
Pre-operative preparation
With the patient in a standing position I evaluate what her size preference is and if she wishes to have projected breasts or small flat ones. I then have an idea of what volume I have to remove and from what area of the breast. This is marked on the breast skin. I also study the areolar position and the natural asymmetries of each patient.
First, I mark the submammary fold. The vertical lines passing through the nipple go to the external notch if I wish to move the areola superiomedially but to the mid-clavicular line if I wish to move the areola superiorly. I then move the areola to the position I think it should be placed, that is, its projection above the future submammary fold, and I mark the superior areola position on the vertical line. According to what I think will be the periareolar skin resection, I mark 5–6 cm on each side of the nipple. This can be 4–7 cm if I wish to move a lateralized areola more medially. From the superior mark to the lateral ones, I then mark a semi-circumference and from there I drop two vertical lines converging 2–4 cm above the SMF. I draw the same mark on the contra-lateral side or I can make different marks if the breast is bigger, smaller or more ptotic.
Technique
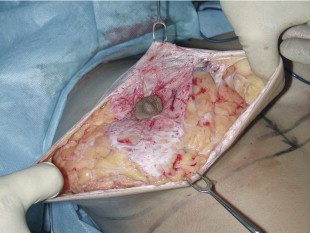
Before beginning the surgery, each breast is thoroughly infiltrated with 250–300 mL of anesthetic solution at the submammary, prepectoralis layer, at the subcutaneous inferior half of the breast skin and under the areola. The anesthetic solution is prepared with 25 mL 2% lidocaine, 25 mL 0.5% bupivacaine, 1 mL 1:1000 epinephrine diluted in 450–550 mL of Ringer’s lactate solution. Once the whole periareolar skin is de-epithelialized, the skin is undermined at the inferior half of the breast medially and laterally, leaving 1 cm thick subcutaneous tissue to preserve its blood supply ( Figure 13.1 ). The inferior half of the breast is also detached from the pectoralis major muscle up to the fourth intercostal space, where the perforant of the fourth intercostal nerve usually emerges ( Figure 13.2 ). In this way, the dissected breast comes out and, holding up the breast with a hook, I mark a w-pattern resection ( Figure 13.3 ), that is at the inferior quadrant and at the inferior part of the medial and lateral quadrants, marking 10 cm distance of what will be the future areola–SMF distance ( Figure 13.4 ).



After the resection, the lateral and medial glandular edges are sutured medially in two to three layers using a 3-0 vicryl suture. In case I want a central projection of the breast, both pillars can be imbricated. To have a more projected breast, two to three stitches are placed at the base of the cone in order to keep the pillars together ( Figure 13.5 ). Once I have obtained a conic shaped breast, the inferior edge of the parenchyma is fixed to the pectoralis facia where it now sits using 5–7 3-0 vicryl separate stitches placed all along what will be the future SMF ( Figure 13.6 ) At this time, some de-fatting can be performed in order to create a more even and round breast shape. I then move the areola to the superior border of the skin and I fix it with two to three subdermal 3-0 vicryl sutures ( Figure 13.7 ). To finish the surgery, a stitch is placed at 8–10 cm from the inferior part of the skin angle, dividing the wound in two figures: the superior round periareolar and the inferior vertical ellipse ( Figure 13.8 ).



Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


