Key points
- •
Where does the no vertical scar technique fit in the armamentarium of reduction/mastopexy techniques relative to the vertical scar and the T scar techniques?
- •
The ideal patient for the no vertical scar technique has a lot of ptosis with at least 5 cm between the areola and the new areolar site.
- •
The main advantages of the no vertical scar technique are a nice periareolar scar with the only other scar hidden in the inframammary fold. There is no vertical scar on the visible breast mound.
- •
The main disadvantages of the no vertical scar technique are the same as those of the T scar: medial and lateral dog ears as well as a possible boxy shape problem if attention is not given to detail.
- •
Intraoperative breast sizers are useful to ensure that remaining breast tissue is of equal volume on both sides before the skin is closed.
Patient selection
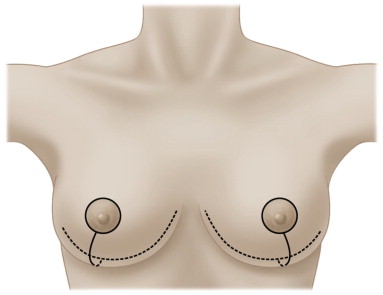
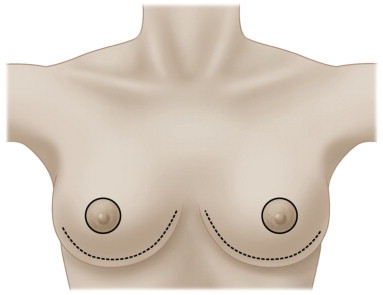
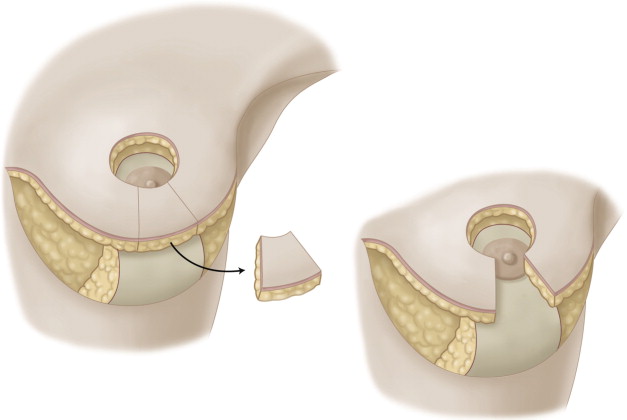
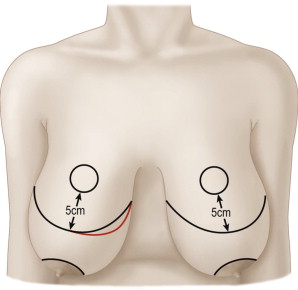
The no vertical scar reduction/mastopexy is essentially the same reliable operation as the T scar inferior pedicle reduction except that it has one less scar; the vertical scar ( Figures 16.1–16.3 ). The most common cause of patient dissatisfaction after breast reduction is the scar ( ). We believe that many patients can achieve a good breast shape with a modification of the T scar operation which deletes the vertical scar. If we can achieve good shape with one less scar than is achieved with a T scar reduction, then why not do it? The most important factor in patient selection for the no vertical scar technique is that the ideal patient is one who has 5 cm or more skin between the areola and the new areolar site ( Figure 16.4 ). In other words, this is a good technique for a patient who has a lot of ptosis and excess skin.
Most surgeons would be reluctant to perform a breast reduction on a patient with a BMI of 45. With regard to obese or overweight patients, most surgeons draw a line somewhere at which point they will not perform the surgery. We calculate normal body weight using standard height/weight tables and give patients the benefit of the doubt using the upper weight deemed appropriate for the largest frames (to account for ‘big bones’). We call all weight above this number ‘pounds of unhealthy fat’, or the patient’s POUF number. We draw the line at a POUF number of 10%. If the POUF number is greater than 10% of the patient’s healthy upper limit body weight, we provide motivational nutritional weight counseling and do not perform the surgery. However, some authors regularly use the no vertical scar technique with good technical results in severely overweight patients ( ).
Indications
Consider for a moment how much skin is removed with the skin excision patterns of the three reduction techniques of T scar, vertical scar reduction, and no vertical scar reduction. The vertical scar reduction has the least amount of skin removal of the three techniques. We therefore prefer the Hall-Findlay vertical reduction/mastopexy for the patient who has less skin to excise, and does not have a great deal of ptosis (less than 5 cm of skin between the areola and the new areolar site). This accounts for approximately 25% of the patients in our practice.
If the patient has a lot of ptosis and skin requiring removal as well as breast, then we prefer the no vertical scar reduction. This accounts for approximately 70% of the patients in our practice. Occasionally a patient will present with an excessively wide breast with a lot of horizontal skin needing excision and in this situation we still sometimes use the T scar reduction (≤5% of our cases). However, most of these patients would also do well with the no vertical scar technique because breast tissue can be made smaller with excision, projection can be obtained with breast shaping sutures, and excess lateral horizontal skin can redrape and become part of lateral chest wall skin no longer overlying the breast.
The no vertical scar technique can be used for either reduction or mastopexy. The Hall-Findlay rotation advancement vertical scar operation (rotation of the medial pedicle superiorly and advancement of the lateral pedicle beneath it) may give more projection than the T scar or no vertical scar techniques. However, breast shaping sutures do augment the projection obtained with the no vertical scar and the T scar techniques ( ).
Operative technique
A film with pre-operative markings and intraoperative technique is available for viewing online at https://www.psvideoworkshop.com/about.htm.
Pre-operative preparation
Markings
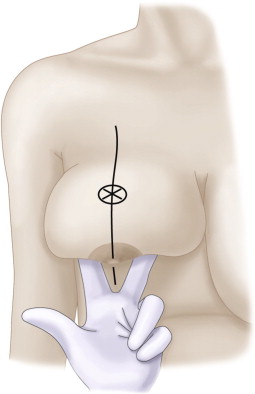
The sternal notch is the first place that is marked. It is easily palpable at the top of the midline sternum between both clavicular heads. A line is drawn down the centre of the breast meridian line where the areola will look best ( Figure 16.5 ). If a large part of the lateral breast is to be removed, the nipple/areola axis line can be moved medially as will be appropriate to the final anticipated breast width. The axis of the breast is drawn as a continued straight line below the inframammary fold by keeping it as a straight line seen through two fingers holding up the breast mound. ( Figure 16.6 )
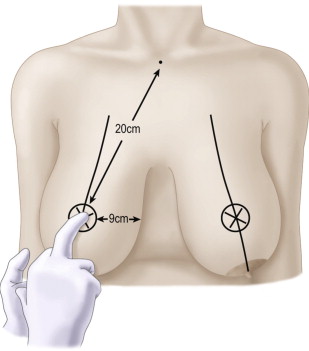
The new nipple site usually ends up between 19 and 22 cm from the sternal notch, and between 9 and 12 cm from the midline. Larger (22 cm) numbers will apply to larger post-operative breasts, and shorter numbers (19 cm) will apply to smaller post-operative breasts. It is better to err on having a nipple too low than too high, as a very high areola may be visible in a low cut bathing suit. A finger on the breast is used to palpate another finger through the breast at the level of the inframammary fold, and this becomes the new nipple site ( Figure 16.5 ). The areolar recipient site skin excision is marked on the skin brassiere pre-operatively with the patient in the sitting position. It is drawn as a slightly horizontal oval (3.5 cm diameter horizontally, and 3.0 cm diameter vertically) as the oval will stretch to a circle when the skin brassiere flap is pulled down over the breast to the inframammary fold at the time of final closure. The areola is marked as a 4 cm diameter circle also with the patient sitting up. The area of the areolar recipient circle is deliberately marked to be a little smaller than the areola itself in order to achieve a tension free closure in the periareolar scar.
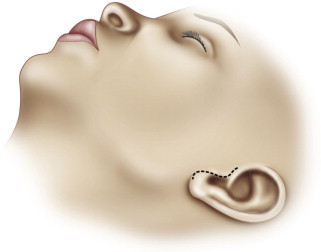
A tension free areolar scar results in a much better areolar scar. This scar is the most visible scar of the reduced breast and the one that the woman will see every day when she is naked ( Figure 16.7 ). It is also the first scar that a significant other will look at when her breast is seen by that person. As it is the showcase scar of the breast it should be treated as we treat the preauricular scar of the facelift; tension free and closed with care ( Figure 16.8 ). The areolar recipient site is deliberately marked a little smaller than the areola itself to get a better tension free periareolar scar when we use the T scar or the vertical scar techniques.

The correct marking of the inframammary fold incision is important. While the vertical reduction has its possible dog ear in the middle of the breast extending to below the inframammary fold, the no vertical scar technique shares the same potential problems of medial and lateral dog-ears and visible scars at the medial and lateral ends of the inframammary fold scars with the T scar technique. To avoid visible medial dog ears in the no vertical and T scar techniques, the medial end of the inframammary fold incision is marked to be hidden under the medial fold of the breast so that it will not be visible post-operatively ( Figure 16.9 ). The medial and central parts of the inframammary incision are drawn in the inframammary fold.










