Key points
- •
The mainstay of transaxillary breast augmentation is the absence of a scar on the breast. It can be adequately performed using endoscopic instruments or even long lightened retractors.
- •
Subfascial breast augmentation offers some advantages over the submuscular placement, without the drawbacks of this approach.
- •
As pectoralis muscle fascia is a well-defined structure and very consistent in the upper thorax, it can be used to cover the implant and minimize visualization of its edges.
- •
Most lymphatic vessels in axilla can be preserved if some technical details of subcutaneous tunnel and pocket dissection were followed.
- •
Subfascial transaxillary breast augmentation has given a no-scar and natural look to the breast. It has also been a reasonable solution to the problem of acquiring adequate soft tissue coverage without distortion of the implant by the muscle contraction.
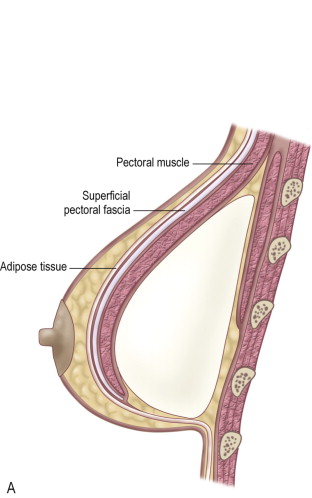
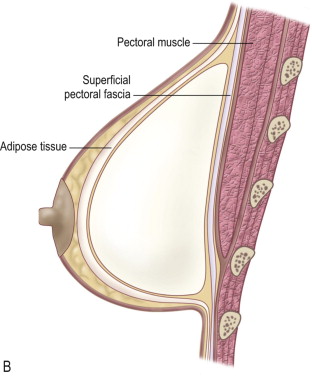
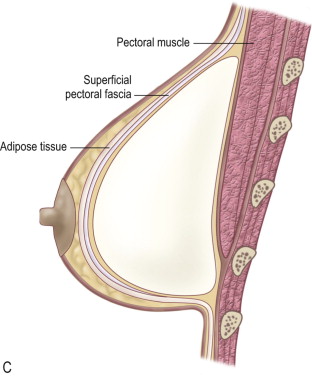
Breast augmentation has been a very common procedure in plastic surgery in the last few decades with multiple options for incision location, implant design and pocket plane. Implant position or pocket plane in breast augmentation has been the subject of some controversy because an implant can be positioned in a subglandular, retropectoral or subfascial plane ( ) ( Figure 7.1 ). For an optimal result, the implant must have adequate soft tissue coverage, otherwise it can become palpable or visible. The position of an implant in a retroglandular space has significant disadvantages if the soft tissue coverage is insufficient.
In addition to implant palpability and visibility, incidences of fibrous capsular contracture, rippling and nipple sensation alteration and numbness are higher ( ). In order to get rid of the problems encountered with retroglandular placement, the utilization of the retropectoral space has become commonplace. The disadvantages of subpectoral placement include a more invasive procedure, increased postoperative discomfort and visible flattening or distortion of the breast when the pectoral muscle is contracted ( ). If the muscle is released inadequately medially the implant may ride too high or if the muscle is released excessively the implant may be displaced inferiorly and laterally.
A reasonable solution to the problem of acquiring adequate soft tissue coverage without distortion of the implant through muscle contracture has been the use of the subfascial plane ( , , ). As the pectoralis muscle fascia is a well-defined structure and very consistent in the upper thorax, it can be used to minimize the appearance of the edges of the implant on the skin, making them less noticeable. The integrity of the muscle is preserved and the implant is totally covered. The fascia supports the implant without requiring additional tissue to give a good aesthetic result. In the subfascial plane, there won’t be any alteration to the breast shape or implant displacement caused by muscular contraction.
The pre-operative evaluation includes the analysis of breast tissue and thoracic shape, the elasticity of the breast, the presence of ptosis, and the distance between the nipple and the inframammary fold. Subfascial breast augmentation aims to offer a better and natural shape to the breast. There is an additional soft, but firm tissue between the implant and skin, which improves breast contour, especially in the upper pole, leading to a less noticable implant edge.
Transaxillary breast augmentation presents many advantages over other techniques ( ). Its mainstay is the absence of a scar on the breast. The rationale for placing the implant submuscularly, and recently subfascially, is to reduce the incidence of capsular contraction in the late post-operative period and to avoid areolar sensation disturbances ( ). The use of endoscopic magnifying lenses and video amplifies the images and gives a better visualization of tissues and planes, allowing more precise dissection and hemostasis while using only a small axillary incision ( , ). This technique is not indicated for moderate and severe ptosis.
Breast endoscopic surgery has been used since 1987, for internal capsulotomy and to evaluate mammary implants ( , , ). In 1993, Johnson and Christ ( ) first described the video endoscopic approach in transumbilical breast augmentation, and in the same year Laurence Ho published his experience with transaxillary endoscopic augmentation ( ). In 1994 Price reported endoscopic transaxillary subpectoral breast augmentation with good aesthetic results and no complications ( ). He was followed by other authors ( , , , ).
Anatomical considerations
The breast is essentially a skin appendage contained within layers of the superficial fascia. The superficial layer of this fascia is near the dermis and is not distinct from it. The deep layer of the superficial fascia is more distinct and is identifiable on the deep surface of the breast when the breast is elevated in a subglandular augmentation mammaplasty. There is a loose areolar tissue between the deep layer of the superficial fascia and the fascia that covers the pectoralis major muscle ( ) and continues to cover the adjacent rectus abdominis, serratus anterior and external oblique muscles ( Figure 7.2 ).

This fascia has its origin on the clavicle and sternum, extending toward the lateral border of the muscle to form the axillary fascia. At the caudal border of the pectoralis muscle, the clavipectoral, pectoral, and serratus anterior fasciae become continuous and form suspensory ligaments that extend to the breast’s inframammary fold ( ). The deep fascia covering the lower aspect of the pectoralis major muscle is well defined, as is the fascia of the serratus anterior muscle. This deep fascia is continuous with the fascia of the external oblique and rectus abdominis muscles. The upper portions of the external oblique and rectus abdominis muscles and their overlying fasciae are deep to the lower portion of the breast. The digitations (spreading) of origin of the external oblique muscle are associated with the lateral inferior fibers of the pectoralis major muscle and laterally with the serratus anterior muscular digitations (spreading). We have observed that the pectoralis major fascia tends to be thin and more fragile over the lower two-thirds of the muscle.
Operative approach
Operative steps:
- •
Skin markings with the patient in upright position.
- •
Important landmarks: inframammary fold (at least 5–7 cm below the areola); medial marking 1–2 cm from the mid sternum; anterior axillary line as the lateral limit.
- •
Subcutaneous infiltration (normal saline + epinephrine 1 : 300,000).
- •
Axillary incision in a natural fold, about 4 cm long, not extended beyond the lateral border of the major pectoralis muscle.
- •
Subcutaneous tunnel dissection should limit inferior-lateral undermining in order to preserve most of lymphatic vessels.
- •
Subfascial breast pocket is created by a blunt or electrocautery dissection.
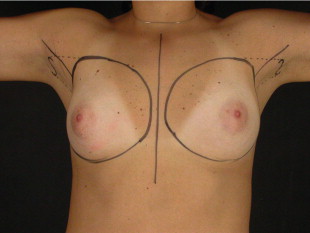
Markings
Pre-operative marking is performed with the patient standing up. The design of the pocket for the implant is marked. The inframammary crease is marked, and if the distance between the areola and the inframammary fold is around 5–7 cm, the original inframammary crease is maintained. However, if this distance is shorter than 4 cm, a new inframammary crease is also marked 1 or 2 cm below the original one. The anterior axillary line is drawn on the lateral side. A line is drawn 1 or 2 cm from the mid-sternum line and extended cephalically to the level of the second intercostal space ( Figure 7.3 ).