Tessier 7—Macrostomia Repair
Patrick A. Gerety
Scott P. Bartlett
DEFINITION
Macrostomia—enlarged oral aperture-related clefting of the oral commissure
Tessier 7 cleft—lateral (transverse) facial cleft from the oral commissure to the zygomaticotemporal suture
Cheilion—anatomic name for commissure point
Commissuroplasty—recreation of oral commissure
ANATOMY1
Oral commissure (FIG 1)
Position
Normal position: at a vertical line dropped from the medial limbus (some variability)
Shape
Normal shape: The upper and lower lip vermilion comes to sharp corner.
Macrostomic commissure: Oblique angle, gaping at rest, round with smile
Tessier 7 cleft resulting in macrostomia
Variable in presentation—may be slightly wider oral commissure or severe cleft of skin, subcutaneous tissue, muscle, and bone
Trajectory—the cleft occurs along a line from the oral commissure to the zygomaticotemporal suture.
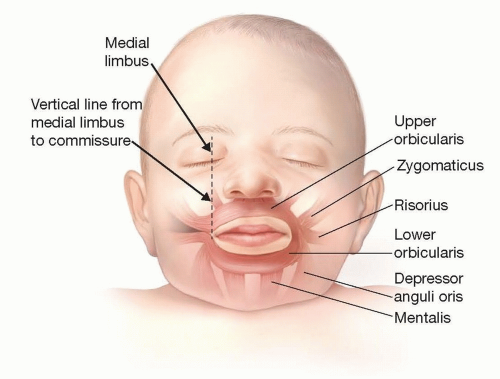
FIG 1 • Lateral facial cleft creates discontinuity of the orbicularis oris at the oral commissure. This in turn affects the location and insertion of the zygomaticus, risorius, and depressor anguli oris muscles.
Affected structures
Commissure—laterally positioned, anatomically abnormal (ie, made of cleft tissue [lighter in color than normal vermilion])
Orbicularis oris—interrupted and malinserted. The superior and inferior limbs contribute to the appearance of the lips on the macrostomic side (see FIG 1).
PATHOGENESIS
Development of normal facial anatomy is dependent upon early first and second branchial arch embryology.
The maxillary and mandibular prominences normally fuse in early embryologic development (weeks 4-6) forming the normal cheeks and lips.
Stapedial artery is the blood supply before the external carotid system has developed.
Stapedial disruption starves all tissue types—skin, fat, muscle, and bone.
Macrostomia results as a presumed failure of this process.
Interruption of embryologic development along the “orotragal” line can affect the oral commissure, muscles of mastication, muscles of facial expression, mandible, maxilla, and auricle.
Isolated macrostomia is a disorder of the first branchial arch only.
NATURAL HISTORY2
Incidence: rare, 1 in 225 000 live births
Unilateral 80%, bilateral 20%
As with cleft lip, the left side appears to be more commonly affected.
May be associated with syndromes including the following:
Hemifacial microsomia
Including Goldenhar syndrome and variants of oculoauriculovertebral spectrum
May account for as many as 25% of macrostomia patients
Treacher Collins syndrome
Auriculocondylar syndrome
Tessier 7: the most common of the rare craniofacial clefts (5%-14%)
PATIENT HISTORY AND PHYSICAL FINDINGS
Laterally displaced oral commissure
Clefted/interrupted orbicularis oris
Oral incompetence may be encountered.
Gaping oral commissure in repose related to cleft orbicularis oris muscle
The cleft margin is demarcated. It does not contain normal lip elements (eg, white roll, dry vermilion), but it is mucosalized. The normal dark red vermilion can be seen to transition into a lighter colored cleft vermilion.
Spectrum of the cleft3
Minor form—1 to 2 cm in length ending medial to the anterior border of the masseter muscle
Major form—cleft ends lateral to the medial border of the masseter. It may terminate at the tragus or at the tonsillar pillar with disruption of superficial and deep structures.
The commissure is blunted/effaced, and when a baby with macrostomia cries, the commissural angle of an open mouth is more oblique than the normally formed commissure—this is thought to be related to disruption of the normally intact orbicularis ring.
Associated anomalies
Preauricular tags
Microtia/ear anomaly
Mandibular hypoplasia
Condylar abnormality
Zygomatic arch abnormality
Hearing loss
IMAGING
3D craniofacial CT—if bony involvement is suspected, this may be obtained to evaluate anatomy.
SURGICAL MANAGEMENT
Trilaminar repair—repair of oral mucosal, orbicularis muscle, and facial skin
Repair consists of
Excision of abnormal cleft margin tissue (mucosa)
Repair/repositioning of orbicularis muscle
Recreation of the oral commissure
Rearrangement of the cutaneous scar to avoid deforming contracture
Repair types (external cutaneous scar):
Straight line
Z-plasty
W-plasty
Preoperative Planning
Standard facial photos should be obtained preoperatively including repose and animated (smiling) if possible.
Appropriate expectations should be created with the parents in terms of realistic commissure appearance and the risk of scar hypertrophy/contracture.
Evaluation for other anomalies and comorbidities with specialist consultation or multidisciplinary team as necessary
3D CT scan if cleft is thought to involve skeletal structures
Timing—as with cleft lip surgery, macrostomia repair may be done early in life. It is also reasonable to delay until late infancy if there is minimal functional or feeding issue. Late treatment reported in the literature is a function of later age at presentation and is usually not due to planned delay in treatment.
Positioning (FIG 2)
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


