Tessier 3 and 4 Clefts (Nasal-Cheek Region)
Philip Kuo-Ting Chen
Vikram S. Pandit
DEFINITION
The Tessier no. 3 facial cleft occurs at the junction of the frontonasal and maxillary process.
It involves the position of an ordinary cleft lip extending upward and passing through the alar base towards the medial canthal region.
The medial part of the eye is displaced laterally and inferiorly (FIG 1A).
The Tessier no. 4 facial cleft is located lateral to the no. 3 facial cleft.
This cleft starts lateral to the philtral ridge and travels lateral to the alar base toward the medial canthal region.
The medial part of the eye is displaced laterally and inferiorly (FIG 1B).
ANATOMY
The Tessier no. 3 and no. 4 facial clefts have similar soft tissue abnormalities resulting in shortened oculo-alar and oculo-oral distances.
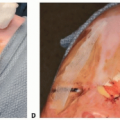
In the lip region, the cleft line is the same as ordinary cleft lip in no. 3 (FIG 2A) and is lateral to the philtral column in no. 4 (FIG 2B).
Both clefts are accompanied by distortion or disruption of the orbicularis oris muscle. The cleft extends upward into the cheek with alar involvement in no. 3 and without alar involvement in no. 4.
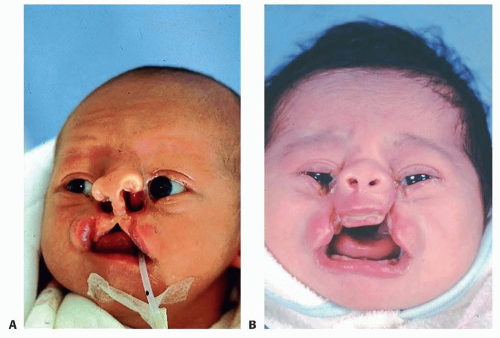
FIG 1 • A. Tessier no. 3 facial cleft. B. Tessier no. 4 facial cleft.
In both clefts, orbital dystopia is coupled with globe abnormalities and underlying skeletal deficiencies.
The medial canthus is displaced inferiorly, and the lacrimal canaliculus on the lower eyelid is usually disrupted.
Usually, it is possible to identify the punctum of the lower eyelid (FIG 3).
There is a coloboma of the lower eyelid (FIG 4).
The involved muscles of facial expression are distorted in their orientation.
The alar base and the lateral part of the nasalis muscle are displaced upward, and the medial part of the cheek muscles is displaced downward.
The underlying maxillary bone is depressed or separated according to the severity of the cleft.
HISTORY AND PHYSICAL FINDINGS
The history taking and physical examination are similar to other patients with craniofacial anomalies.
The history should include the family history, medications during the first trimester, and prenatal diagnosis.
Physical examination should include the extent and location of soft tissue cleft, eye condition, involvement of alveolus, palate, and also other associated systemic problems.5
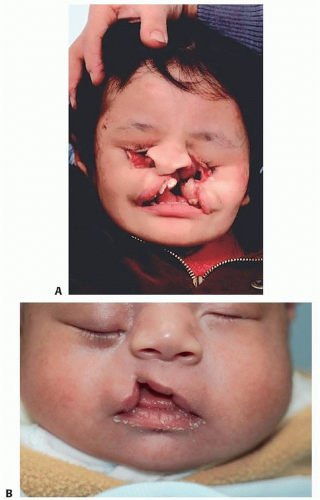 FIG 2 • A. The cleft lip of a Tessier no. 3 is similar to an ordinary cleft lip. B. The cleft lip of a Tessier no. 4 is lateral to the philtral column. |
IMAGING
Radiographic images are usually not necessary in the first visit.
CT scanning is helpful to determine the extent of bony defect on orbital floor if the patient has severe orbital dystopia (FIG 6).
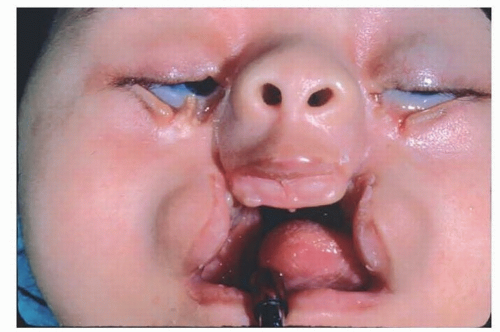
FIG 3 • The punctum can be identified lateral to the cleft.

FIG 4 • Coloboma of left lower eyelid.
Panoramic x-rays and CT scans are also helpful to evaluate the necessity of bone grafting in the alveolar or cheek region when the patient is older (FIG 7).
In the author’s center, cephalometric and panoramic radiographs and CT scans with 3D reconstruction are routinely recorded every 2 years from ages 5 to 17 years to monitor facial growth.
SURGICAL MANAGEMENT
Surgical correction of the soft tissue problems is undertaken between 3 to 6 months of age. This correction should aim at the restoration of normal facial appearance and protection of the eye.
Bony reconstruction of the alveolar clefts is similar to the timing of alveolar bone grafting in cleft patients, ie, in the mixed dentition period before the eruption of the teeth in the cleft region.
The bony reconstruction for the skeletal defects on the face and orbit is generally not undertaken till the patient is at least 3 years of age and more commonly at the age of 5 years.
This allows the inner and outer tables of the calvarium to be split and therefore obtain a large amount of bone graft with minimal donor morbidity.
However, when there is severe bony deficiency on the orbital floor causing a significant dystopia of the globe, orbital floor reconstruction should be considered at an earlier age.
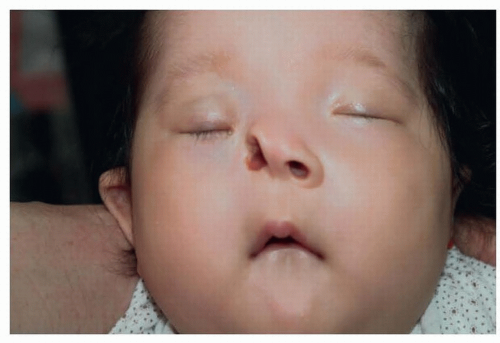
FIG 5 • Tessier no. 3 cleft with cleft on cheek region and intact lip.
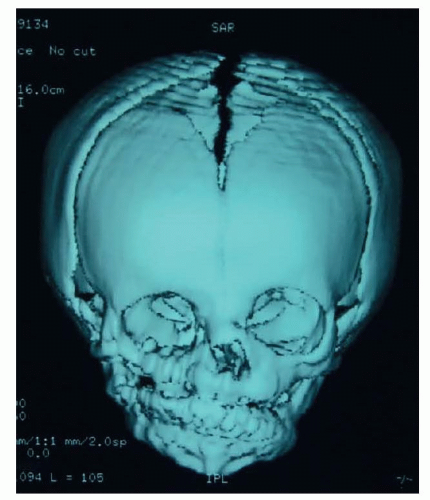
FIG 6 • 3D CT scan of a right Tessier no. 4 facial cleft.
The repair of the soft tissue deficit in the Tessier no. 3 and no. 4 craniofacial clefts is based on five basic components as outlined.6
A medial canthopexy with 2 mm overcorrection in an upward vertical position
The postoperative scar contracture will always pull the new medial canthus inferiorly.
Midface rotation advancement is performed with rotation of the medially based nasal flap, advancement of the laterally based cheek flap, and repositioning of the facial muscles.
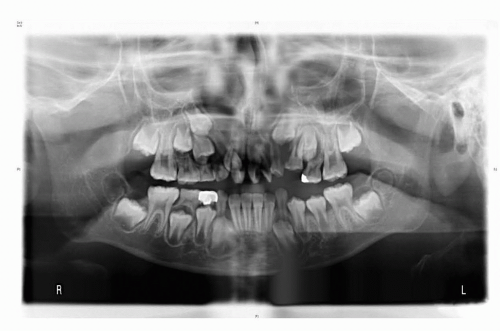
FIG 7 • Panoramic radiograph of a bilateral Tessier no. 4 facial cleft.
This helps to lengthen the shortened oculo-oral and oculo-alar distances while restoring normal facial expression.
This is similar to the rotation-advancement repair in ordinary cleft lip.
The lengthening achieved in the midface region should primarily be due to muscle repositioning rather than skin Z-plasties.
Placement of the surgical scars should be along the junction of the facial units, rather than placing multiple Z-plasties on the cheek, to avoid color mismatching due to skin differences in the nasal and cheek regions.
Placement of the scar lateral to the junction of the facial units will result in visible scars on the cheek region.7,8,9,10,11Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree