Chapter 54 Tensioning Anterior Cruciate Ligament Grafts
Introduction
Graft selection, graft position, fixation, and postoperative rehabilitation are clearly implicated in the success and failure of anterior cruciate ligament (ACL) reconstruction. Tensioning of the ACL is another important factor in providing immediate and long-term stability in the reconstructed patient. Jones1 stated that tension applied to the ACL graft at the time of surgery should be enough to eliminate an anterior drawer sign but still allow a full range of motion. Excessive initial tension can lead to graft failure, fixation failure, loss of knee motion, excessively reduced anterior laxity, and cartilage degeneration.2–6 Lewis et al6 introduced the term overcorrected to describe the phenomenon in which the tibia was positioned posterior and externally rotated relative to the femur. Andersen and Jorgensen7 used a prosthetic ligament to study the consequence of overcorrected ACL reconstructions. These kinematic alterations result in increased graft forces at all flexion angles, increased forces in the posterior cruciate ligament (PCL), and alteration of the normal roll–glide mechanism during knee motion. Melby et al2 found that graft tension–related posterior tibial subluxation resulted in an increase in quadriceps force needed to achieve full knee extension and may lead to an extensor lag if quadriceps atrophy is present.
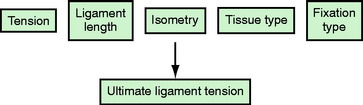
Initial tension affects the biology of the graft and is a time-dependent interplay of host incorporation and biomechanical forces. A number of factors affect graft tension, including initial tension (pretensioning and preconditioning), ligament length, graft isometry, tissue type, and fixation type (Fig. 54-1). For the purposes of this chapter, we will review the consequences of overtensioning the ACL graft both histologically and functionally, explore the factors in low-tension (bone–tendon–bone [BTB]) and high-tension (soft tissue) grafts, identify the ideal knee fixation angle, and provide suggestions for identifying tensioning problems and possible solutions. Historically, much debate has existed in the literature regarding these issues, with relatively few clinical studies focusing on graft tension; however, some consensus has been identified in recent years to lend clarity to this confusing topic.
Native Anterior Cruciate Ligament Tension
The goal of ACL reconstruction is to restore normal knee kinematics. Success requires a basic understanding of the forces affecting the normal ACL. Markolf et al8 and Wascher et al9 studied a series of loading experiments on cadaver specimens by isolating the bone plug that contained the ligament’s tibial insertion and attaching a load transducer. Passive extension of the knee generated forces in the ligament only during the last 10 degrees of extension, reaching 50 to 240N with hyperextension. Internal tibial torque generated greater forces in the ligament than did external tibial torque and increased as the knee was extended. The greatest forces (133–370N) were generated when 10 N/m of internal tibial torque was applied in hyperextension. A varus moment of 15 N/m generated forces of 94 to 177N at full extension, and a similar valgus moment generated a mean force of 56N independent of knee flexion.
Active knee motion near extension substantially increases forces across the ACL. Paulos et al10 reported that lengthening of the ACL was observed during active extension from 40 degrees of knee flexion. Active quadriceps contraction imparts significant strain on the ACL. Arms et al11 showed that over the first 45 degrees of flexion, the quadriceps increased strain, whereas it decreased strain at flexion angles greater than 60 degrees. Beynnon et al12 studied the forces on the anteromedial bundle of various exercises. Isometric quadriceps contraction at 15 degrees of knee flexion elicited the highest peak strain (4.4%), followed by open chain flexion-extension with a 45N weight (3.8%) and a Lachman test (3.7%). Isometric quadriceps contraction at 30 degrees contributed significantly less strain (2.7%) to the ACL.
More recent investigation has focused on the importance of both the anteromedial and posterolateral bundles in ACL function. Sakane et al13 examined in situ forces in nine human ACLs in response to applied anterior tibial loads at knee flexion angles of 0 to 90 degrees. Their results showed the magnitude of ACL force to be maximal with anterior tibial loads applied at 15 degrees of knee flexion, which differs slightly from Markolf’s earlier conclusions. The magnitude of force in the posterolateral bundle was larger than that in the anteromedial bundle at knee flexion angles between 0 and 45 degrees, reaching a maximum of 75N at 15 degrees of knee flexion under an anterior tibial load of 110N. The magnitude of force on the anteromedial bundle, in contrast, remained constant independently of flexion angle. They concluded that the magnitude of force in the posterolateral bundle was significantly affected by knee flexion angle and anterior tibial load and was the major restraint to anteroposterior (AP) instability in early flexion.
No graft currently in use matches the complex anatomy of the normal ACL. Woo et al14 compared anteromedial ACL reconstructions using hamstring and patellar tendon reconstructions versus the native ACL and found significant laxity to a combined rotational load involving internal rotation and valgus tibial torque at 15 and 30 degrees of flexion. This highlights the importance of the posterolateral bundle to knee stability in early knee flexion and has led some to question the anteromedial reconstructions and revisit the idea of anatomical double-bundle reconstructions.
Basic Science and Graft Histology
Evidence from animal experiments lends credence to a “window” of acceptable ACL graft tension. Graft tension that is too high can eventually lead to greater laxity and poorer results than knees fixed under low graft tension. Conversely, other animal studies demonstrate that deliberately de-tensioned grafts lose strength to a greater extent than the normally tensioned ACL. Although a stimulus is essential for the orientation of newly formed collagen during the remodeling phase,15 basic research studying the effect of graft tension cautions that high initial tension may be detrimental to the remodeling process. Yoshiya et al16 found that patellar tendon reconstructions in dogs exposed to high initial graft tension of 39N showed focal degeneration within the graft and replacement of the normal parallel arrangement of collagen fibrils by a myxoid, extracellular matrix. Microangiography demonstrated improved vascularity when the initial tension was 1N rather than 39N. Laxity measurements of the two different preloads showed increased stability of the highly tensioned graft at time zero. However, at 3 months, laxity between the two groups was similar.
The use of allograft tissue is gaining popularity in ligament reconstruction. The substantial decrease in graft strength during initial phases of healing in frozen allograft tissue relates to the inflammatory stages associated with revascularization, not the effects of freezing itself.17 Jackson et al18 studied the biomechanical outcomes of devitalized ACL at 0, 6, and 26 weeks after treatment with a freeze probe. At 6 weeks a significant reduction in maximum load to failure was observed. However, at 26 weeks, no differences were noted between frozen and contralateral controls relative to laxity, load to failure, stiffness, or modulus of elasticity.
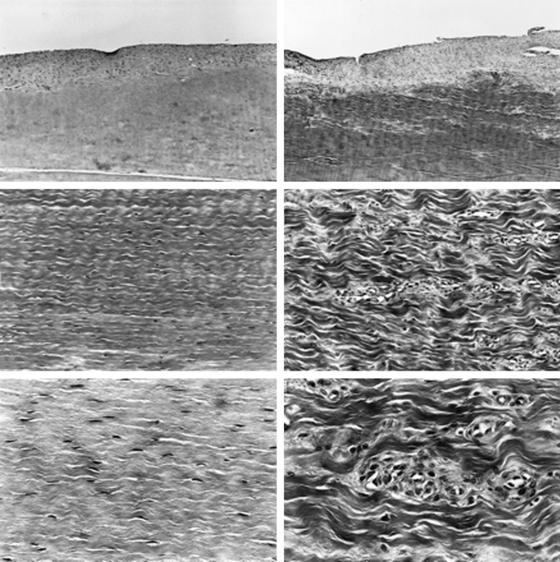
Katsuragi et al19 and Mikami et al20 studied nonphysiologically high initial tension after freezing ACL ligaments in dogs. After applying a freeze-thaw treatment to both ACLs, they applied initial tension of 20N to the test group and compared it with the physiologically tensioned contralateral extremity. The tensile strength in the highly tensioned knee decreased significantly at 6 and 12 weeks. Histologically, the collagen fibers in the highly tensioned knees were coarser and disoriented. In the midsubstance of the ACL, the physiological specimens had a spindle-shaped nucleus; however, the highly tensioned ACL had signs of degenerative changes (Fig. 54-2). Overtensioning causes significant degenerative changes in native, autologous BTB, and freeze-thaw–treated ACL. Over time, the mechanical properties of the overtensioned ACL graft deteriorate compared with physiological tension.
Graft-Specific Tensioning
Stiffness and elasticity vary among autograft tissues. Burks and Leland4 determined that the graft tension needed to restore normal anterior laxity is tissue specific. The material (stiffness) and geometrical (size and length) properties of the graft influence the amount of tension that needs to be applied. In cadaveric knees, they reconstructed the ACL using bone–patellar tendon–bone (BPTB), doubled semitendinosus, or iliotibial band grafts. They tensioned each graft to match translation of an applied 20-pound load (89N) using the KT-1000. The BPTB graft returned the knee to its preoperative condition with a mean of 3.6 pounds (16.2N); doubled semitendinosus graft, 8.5 pounds (38.3N), and iliotibial band graft, 13.6 pounds (61.2N). Due to the characteristics of BTB graft superstructure and fixation, they have been generalized as low-tension grafts, whereas the mechanical properties of soft tissue grafts have necessitated high tension for graft fixation. We will review some of the clinical evidence supporting this.
Low-Tension Grafts
Fleming et al21 studied the relationship between graft tensioning and AP laxity of the reconstructed goat knee. The AP laxity values of the intact knee were measured with the knee at various flexion angles. The ACL was then severed and the laxity measurements were repeated for nine different tensioning conditions: 30N, 60N, and 90N, each applied with the knee at 30, 60, and 90 degrees of flexion. They concluded that a 60N load applied at 30 degrees was the best combination for restoring normal AP laxity values. Pena et al22 developed a three-dimensional finite element model of the human knee joint. Under an anterior load of 134N, the closest anterior tibial translation to that of the intact knee was obtained with a pretension of 60N. However, they noted that because this load was likely to cause problems in revascularization and remodeling during postoperative healing, an initial tension of 40N was recommended.
There is no consensus for the ideal initial tension in BTB graft in clinical studies. Van Kampen et al23
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


