Acknowledgments
The authors would like to acknowledge the generous assistance of Mr Donald Sammut in the preparation of this chapter.
 For video accompanying this chapter see ExpertConsult.com . See inside cover for access details.
For video accompanying this chapter see ExpertConsult.com . See inside cover for access details.
Introduction
Tendon transfer is the surgical transplantation of a normal muscle–tendon unit (MTU) into a new location to restore function of a nonfunctioning MTU. This may be distinguished from a tendon graft, as in tendon transfer the donor tendon remains connected to its native muscle.
In 1770 Missa, a French surgeon, repaired a middle finger extensor tendon injury by grafting the index and ring finger extensor tendons to the middle finger extensor tendon, thus performing the first recorded tendon transfer. However, the modern technique of tendon transfer as defined above was pioneered by Carl Nicoladoni in 1881, and further developed by Tomasz Drobnik with particular reference to radial nerve palsy in 1894.
There was subsequently a dramatic expansion in the number and use of tendon transfer techniques by surgeons such as Bunnell, Brand, and Boyes ( Fig. 49.1 ), faced with the polio epidemics and war injuries of the early 20th century. In this chapter we present the approach of the senior author (S.F.) to tendon transfers in the upper limb for peripheral nerve injury and tetraplegia. See Table 49.1 for definitions of terms used in this chapter.

|
Indications
The essential indication for tendon transfer is the functional impairment of an MTU, either through direct injury, denervation, or developmental abnormality of muscle ( Table 49.2 ). Specific indications for tendon transfer are delayed presentation or direct injury resulting in loss of tendon length rendering primary repair impossible, direct nerve injuries not amenable to repair, late presentation of nerve injury with motor endplate fibrosis, failed nerve transfers, plexus injuries, nerve root avulsions, spinal cord injuries, central neurological insults, and certain congenital or developmental disorders.
|
Burkhalter has also advocated the use of early tendon transfer as an adjunct to nerve repair to retain function and reduce development of contractures during nerve recovery. Such a transfer serves to improve function during nerve regeneration, reducing the need for external splinting, supplements the power of the muscles being reinnervated, and may serve as a definitive procedure where nerve regeneration is limited. However, such transfers should not themselves cause significant loss of function, or result in deformity following recovery of function in the affected nerve.
Biomechanics
The majority of tendon transfers performed routinely are known to be based on sound biomechanical principles. However, an understanding of basic biomechanics is helpful for the surgeon, particularly when faced with a difficult case where the standard approach may not be feasible. The ultimate aim of a tendon transfer is the creation of a new MTU capable of generating torque sufficient to move a target joint through a useful range of motion. Torque is determined by the power, or force-generating ability, of the muscle, and its mechanical advantage, or leverage. Other relevant biomechanical characteristics are the degree of tendon excursion, and tensioning of the muscle during transfer.
Power and Leverage
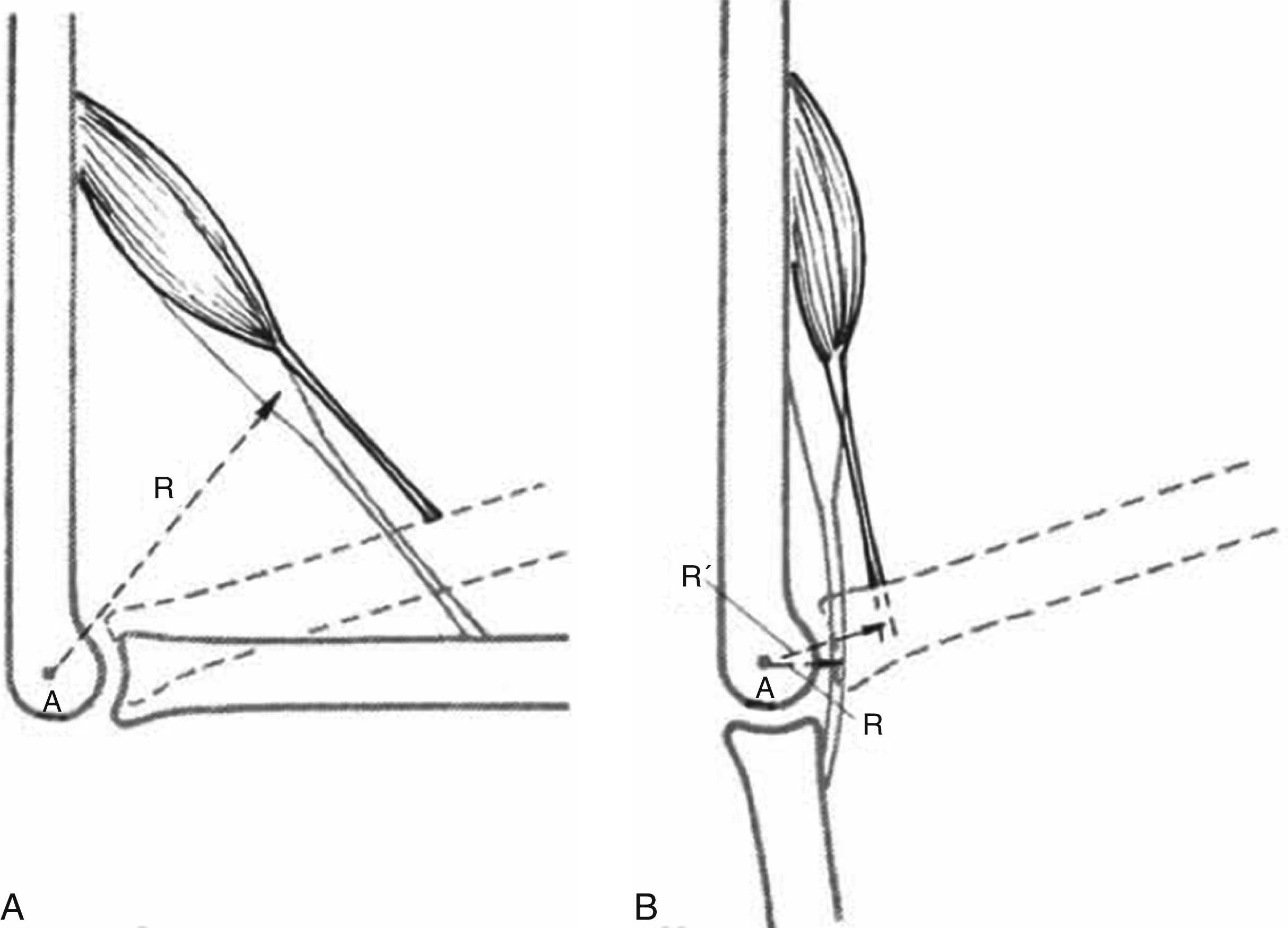
The power, or force-generating ability, of a muscle is proportional to its physiological cross-sectional area (PCSA). Leverage is a measure of the mechanical advantage of a muscle. It is determined by the moment arm, which is the perpendicular distance from the target joint’s axis of rotation to the line of pull of the muscle ( Fig. 49.2 ). It should be noted that the moment arm may vary depending on joint position, and any measurements should be taken with the joint in a useful position. Muscles with a larger moment arm have relatively more leverage, and hence exert greater torque. For an MTU to be useful for a transfer, it must have adequate power and leverage to move the target joint.
Tendon Excursion
Excursion is the distance a tendon can move from when it is relaxed to its fully contracted position. Tendon excursion and contraction velocity are proportional to muscle fiber length. An appropriate donor MTU must have adequate excursion to move the target joint through a useful range of motion. The moment arm is again relevant here (see above). As the moment arm increases, the amount of joint movement produced by a given amount of tendon excursion decreases. Hence, adjusting the moment arm of a transferred MTU is a tradeoff between range of motion and leverage.
Tensioning
Normal contraction of an MTU requires overlap of actin and myosin filaments in the sarcomeres of the muscle fibers. An excessively tight or loose muscle will not contract effectively, as is expressed by the Blix curve. Hence, it is critical for the surgeon to put the transferred MTU under appropriate tension. It has been suggested that it may be preferable to place the transferred MTU under excess tension, relying on postoperative relaxation and lengthening to correct any errors. However, studies have demonstrated that this may overestimate the degree to which the muscle may remodel to accommodate its new length and result in a significant loss of muscle power. Ultimately, the surgeon should aim to neither over- nor undertension the transferred MTU by setting it as close to its optimal length as possible. However, this is not easy to establish intraoperatively, as the muscle’s slack length once it has been released from its insertion is not reliably related to its optimal length. Nevertheless, an on-table estimate of the tension on a transferred tendon remains the usual method of determining the amount of tension to put on the transferred MTU. The senior author uses a comparison of distance from MTU origin to previous and new insertion as a guide.
Principles
General principles guiding tendon transfer have been developed and refined since the early 20th century. It should be borne in mind that these are not strict rules that need to be followed in all cases ( Table 49.3 ). For example, though Steindler proposed that the “gliding apparatus” of the tendon should be preserved or reconstructed as much as possible, to minimize the risk of adhesions developing, this is not possible for every patient. However, if the transferred tendon’s course passes through scarred, inflamed, or edematous tissues, then it may be desirable to revise the soft tissue bed using flaps or grafts prior to transfer. Nevertheless, these principles are useful guidelines for both assessing patients’ suitability for tendon transfers, and also in selecting the best procedure for an individual patient.
|
General Approach
Patients presenting with peripheral nerve palsies should have a comprehensive history taken, recording the symptoms, etiology, time course, and any investigations or procedures performed. A complete neurological examination is required to document the motor and sensory deficit. The limb should be further assessed for soft tissue injuries, especially for any areas of scarring, edema, or inflammation along the path of any tendon transfers.
Measurements of the passive and active range of motion of all affected joints should be taken. Further imaging and investigation by means of nerve conduction studies and electromyography may be performed where the diagnosis of the original injury is not clear, or to identify potential confounding anatomical variants such as Martin–Gruber, Marinacci, Riche–Cannieu, and Berretini anastomoses. Once the problem has been clearly defined, reconstruction may be planned.
It is the senior author’s preference to wait for neurological recovery to plateau prior to considering tendon transfers. Based on the works of Sunderland and Seddon, nerve regeneration progresses at approximately 1 mm a day. Depending on the location of the injury, this may mean delaying surgery for 12–18 months.
Surgical Technique
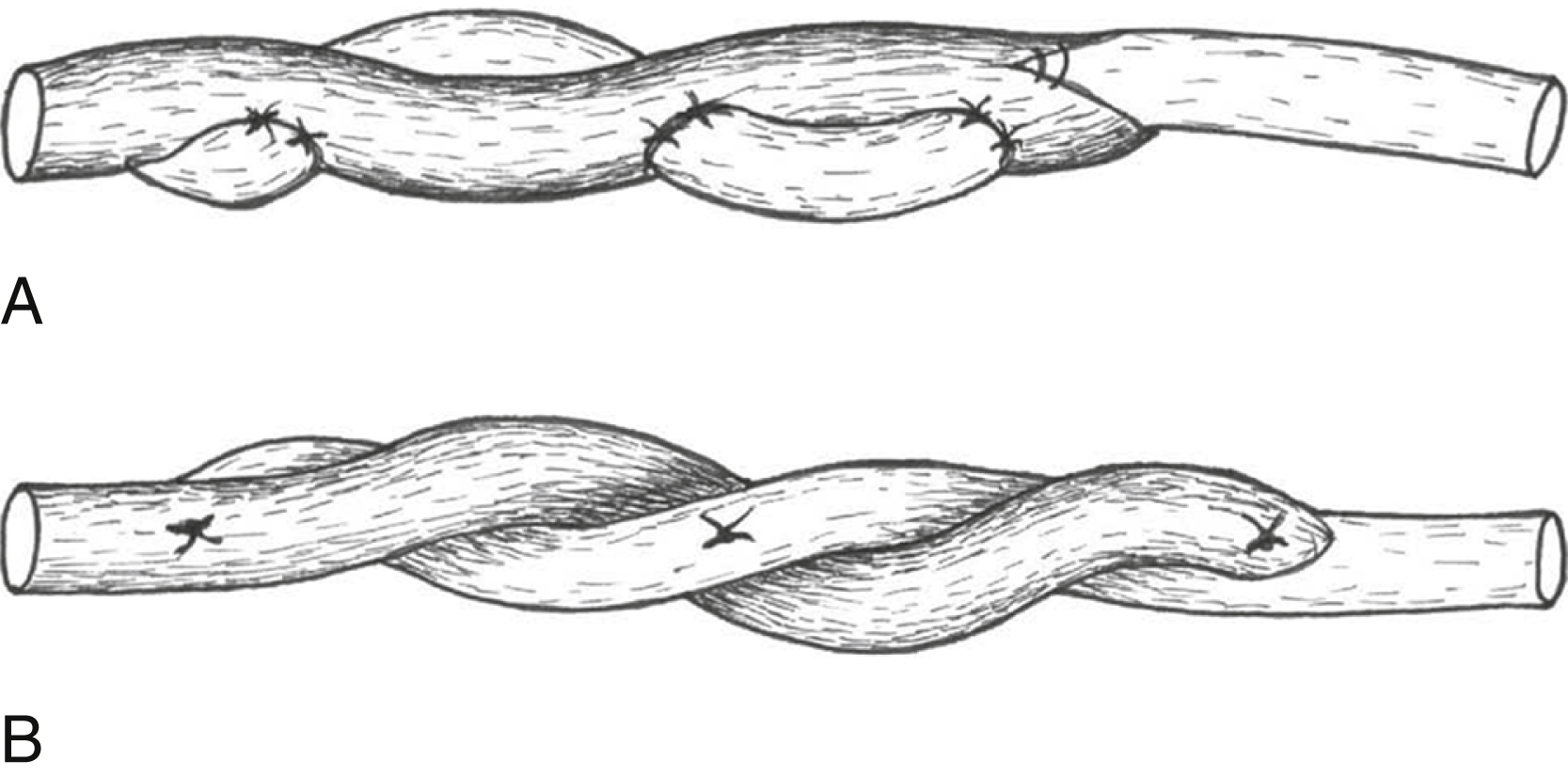
A number of different techniques have been developed for the coaptation of tendons. The Pulvertaft weave, Kessler grasping suture, and Mason/Nicoladoni side-to-side repair have all been used historically. Recently, newer alternatives have been developed, such as the lasso and spiral linking repairs, which demonstrate comparable strength and may be easier and quicker to perform. The senior author’s preference is to use the Pulvertaft weave ( Fig. 49.3 ).
Radial Nerve Palsy
Anatomy , ,
The posterior cord of the brachial plexus continues as the radial nerve after having given off its terminal branches in the axilla. It comprises motor and sensory fibers from the ventral rami of C5 to T1. While in the axilla it gives off its first two branches to triceps, to the long and medial heads. It crosses the lower border of teres major to enter the anterior compartment of the arm and immediately dives into the posterior compartment via the triangular interval. It then runs in the spiral groove (aka radial groove) of the humerus. While in the posterior compartment it gives its last two branches to triceps, one to the lateral head, and a second to the medial head, as well as two sensory branches: the lower lateral and posterior cutaneous nerves of arm. Approximately halfway down the arm the radial nerve pierces the lateral intermuscular septum to re-enter the anterior compartment of the arm. Here it gives off a medial branch to brachialis and lateral branches to brachioradialis and extensor carpi radialis longus (ECRL). It then enters the cubital fossa under cover of brachioradialis, before dividing into deep and superficial branches. The deep branch passes between the two heads of supinator to become the posterior interosseous nerve, while the superficial branch continues down the anterior compartment of the forearm under cover of brachioradialis. The posterior interosseous nerve immediately divides into branches to the extensor musculature of the forearm. The superficial branch of the radial nerve emerges on the radial side of brachioradialis at the wrist to cross the anatomical snuffbox and provide the sensory supply to the dorsum of the hand and the radial three and a half digits.
Clinical Findings
The characteristic sign of radial nerve palsy is wrist drop. Due to the loss of the extensor musculature of the forearm, the patient is unable to extend the wrist or digits. In addition, grip strength is lost due to the weakness of finger flexion with the wrist in a flexed position. Low radial nerve lesions are defined as those below the elbow, thus sparing supply to brachioradialis and ECRL. In these cases, wrist extension is relatively preserved, though with radial deviation. Due to the proximal origin of the majority of the branches of the radial nerve, triceps function is only affected in very proximal lesions. The sensory deficit of radial nerve injury is less significant, only affecting the less sensitive dorsum of the hand and radial three and a half fingers.
Approach , ,
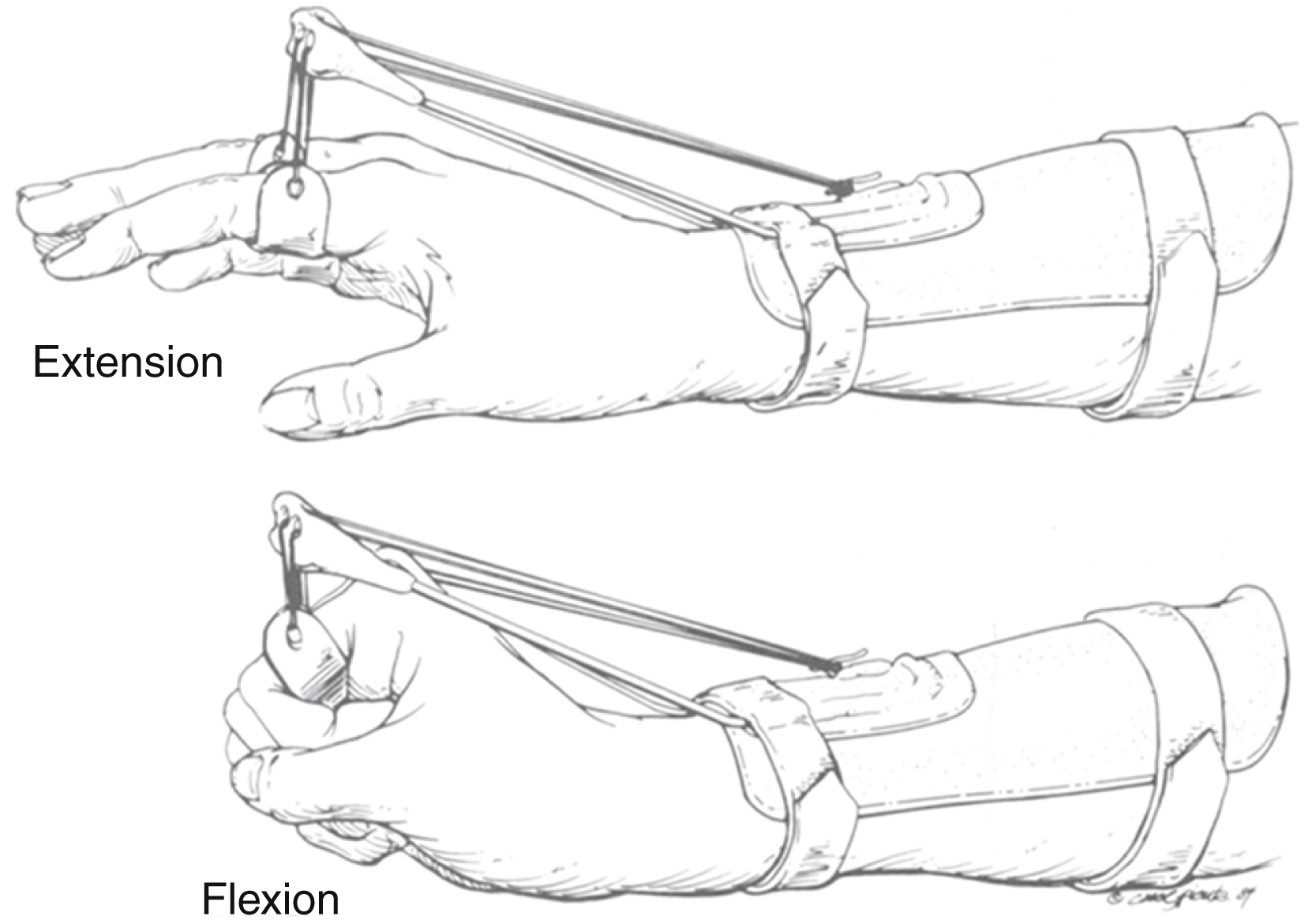
The key reconstructive aims are: wrist extension, metacarpophalangeal (MCP) joint extension, and thumb extension and abduction ( Table 49.4 ). These are generally performed in set combinations for ease of access and operative technique, with the main difference being the choice of MTU to be used for restoration of MCP joint extension. As discussed above (see Indications), some authors advocate using an early tendon transfer procedure to preserve function and prevent contractures in cases of radial nerve injury. Where this is not done, the use of a dynamic outrigger splint ( Fig. 49.4 ) results in greatly improved grip strength by fixing the wrist in extension.
| Reconstructive Aim | Preferred Options | Alternatives |
|---|---|---|
| Wrist extension | PT → ECRB | Rarely consider BR (if function preserved) or FCR → ECRB |
| Metacarpophalangeal joint extension | FCR → EDC (Starr, Brand, Tsuge) | FDS → EDC (Boyes, Chuinard) FCU → EDC (Jones) |
| Thumb extension and abduction | PL → EPL | Ring finger FDS → EPL (Boyes) |
Wrist Extension
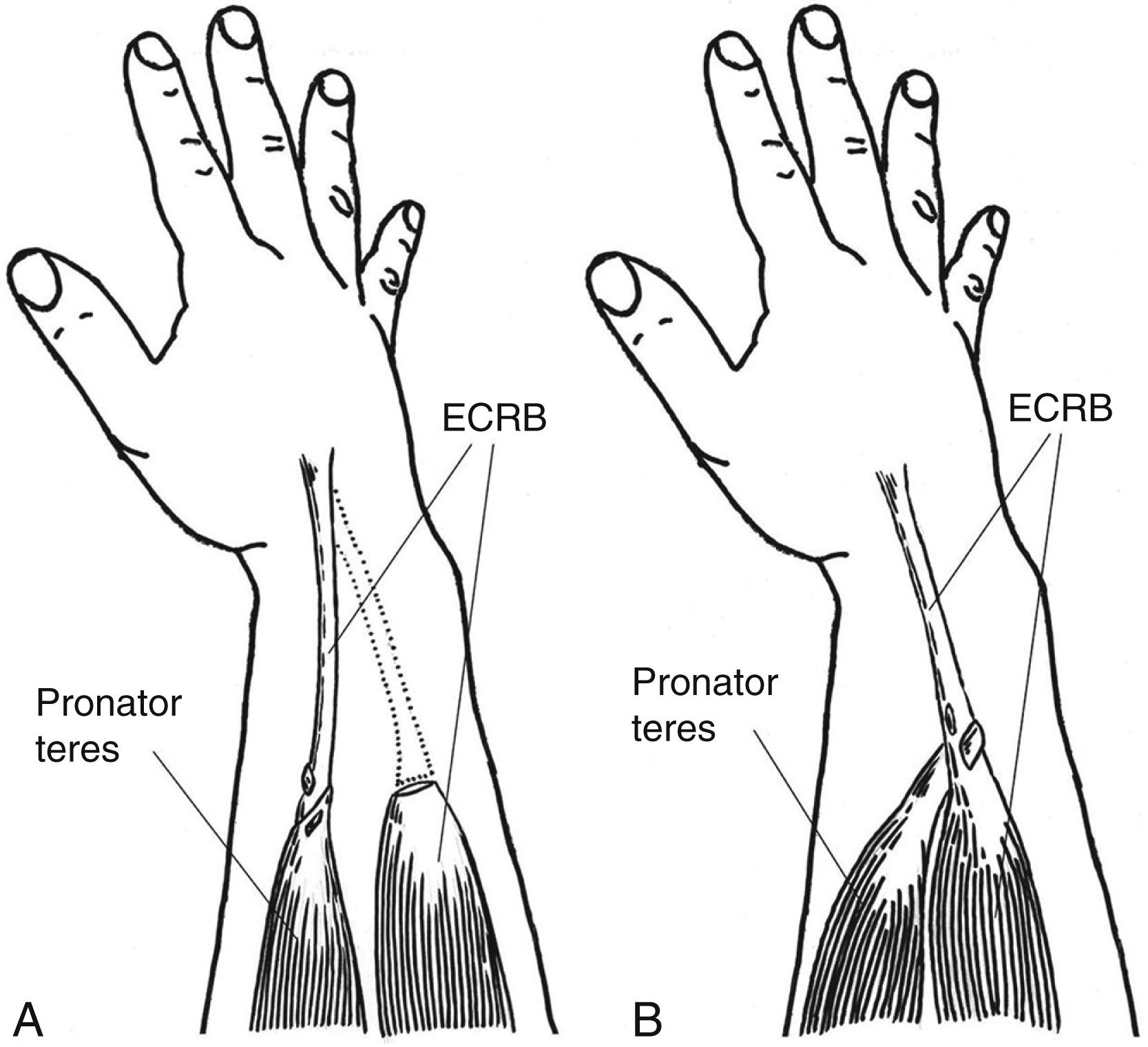
For reconstruction of wrist extension, the pronator teres (PT) to extensor carpi radialis brevis (ECRB) transfer is ideal ( Fig. 49.5 ), and other options are rarely considered. If radial nerve recovery is not anticipated, this should be performed end-to-end to achieve a more direct line of pull. If radial nerve recovery is anticipated, the transfer should be performed by an end-to-side technique, to allow ECRB to resume wrist extension once it regains function. PT should be released from its insertion with a strip of periosteum to provide a robust attachment. It is tunneled subcutaneously superficial to brachioradialis and ECRL, and inserted into the tendon of ECRB. If desired, ECRL may be synchronized to ECRB, with PT redirected to the new extensor complex.
Metacarpophalangeal Joint Extension
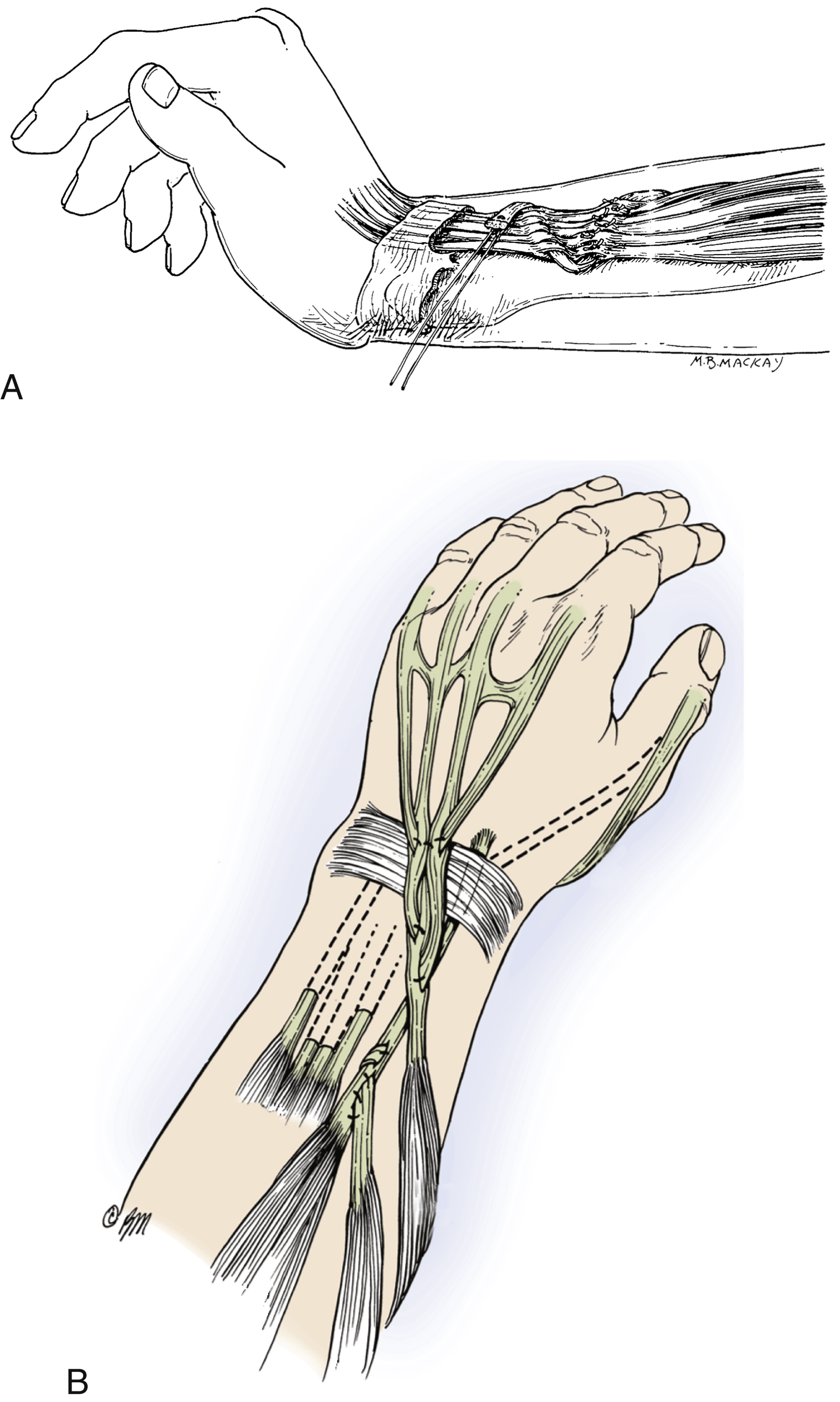
To restore MCP joint extension, a tendon transfer to extensor digitorum communis (EDC) is required. The surgeon is presented with a number of alternatives for this purpose (see Table 49.4 ). Of these, the flexor carpi radialis (FCR) transfer is generally preferred in low radial nerve palsy ( Fig. 49.6 ), as its loss is balanced on the radial side of the wrist by the preserved function of ECRL. By comparison, use of the flexor carpi ulnaris (FCU) transfer necessitates sacrifice of the only remaining muscle acting on the ulnar side of the wrist, resulting in radial deviation. However, both of these transfers suffer from the major drawback of having relatively low excursion for their intended function. For this reason, flexor digitorum superficialis (FDS) transfer as described by Boyes is sometimes preferred, as it has significantly greater excursion, allowing full extension of the digits without requiring wrist flexion. Whichever donor is used, it may be attached to EDC either by leaving it in continuity, or by dividing the tendons of EDC to allow end-to-end attachment of the transferred tendon. If the tendons are divided, they may be passed superficial to the extensor retinaculum to optimize the line of pull.
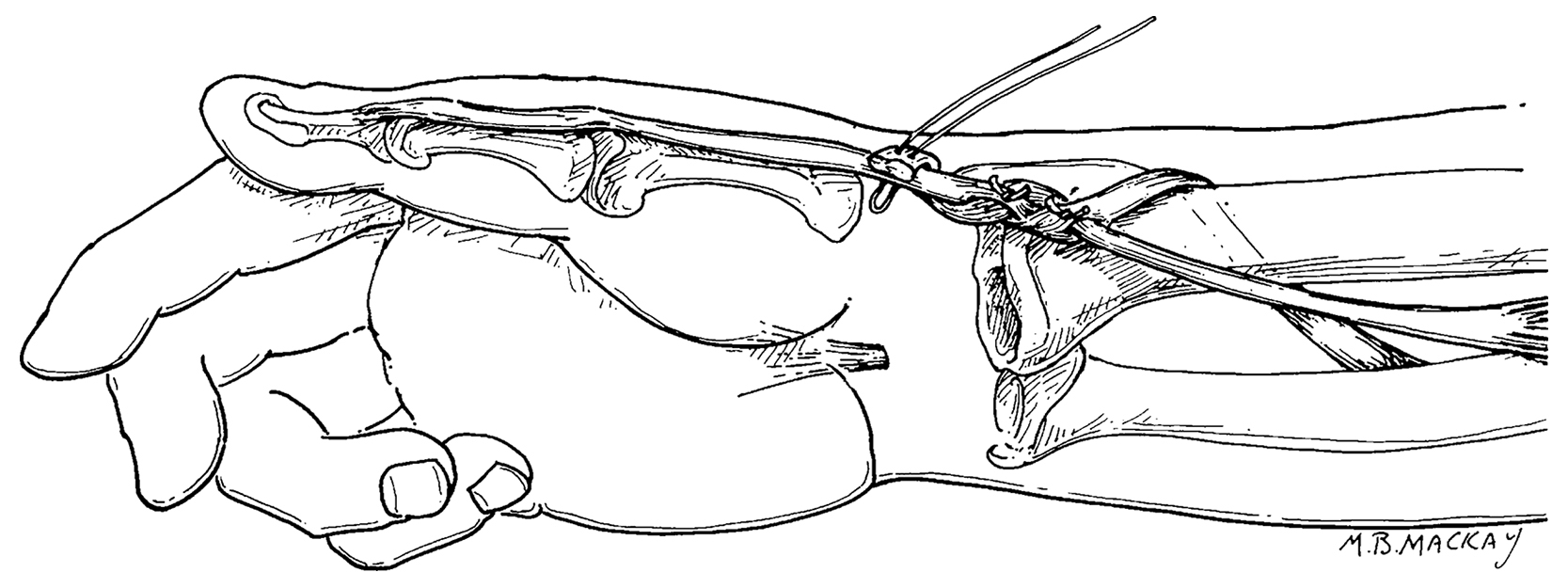
Thumb Extension
Extensor pollicis longus (EPL) is the common target for tendon transfers to restore thumb extension. It is divided at its musculotendinous junction and transposed to the radial aspect of Lister’s tubercle. PL is divided at the wrist and freed up proximally, passed over the radial side of the wrist, then inserted into the distal stump of EPL ( Fig. 49.7 ). The line of pull of the transferred tendon should cross the anatomical snuffbox, resulting in combined extension and abduction with muscle contraction. An alternative is to use the ring finger FDS tendon to power EPL. This is usually done during a Boyes transfer, when other parts of FDS are also being transferred to extensor indicis (EI).