Tendon Transfers
Description
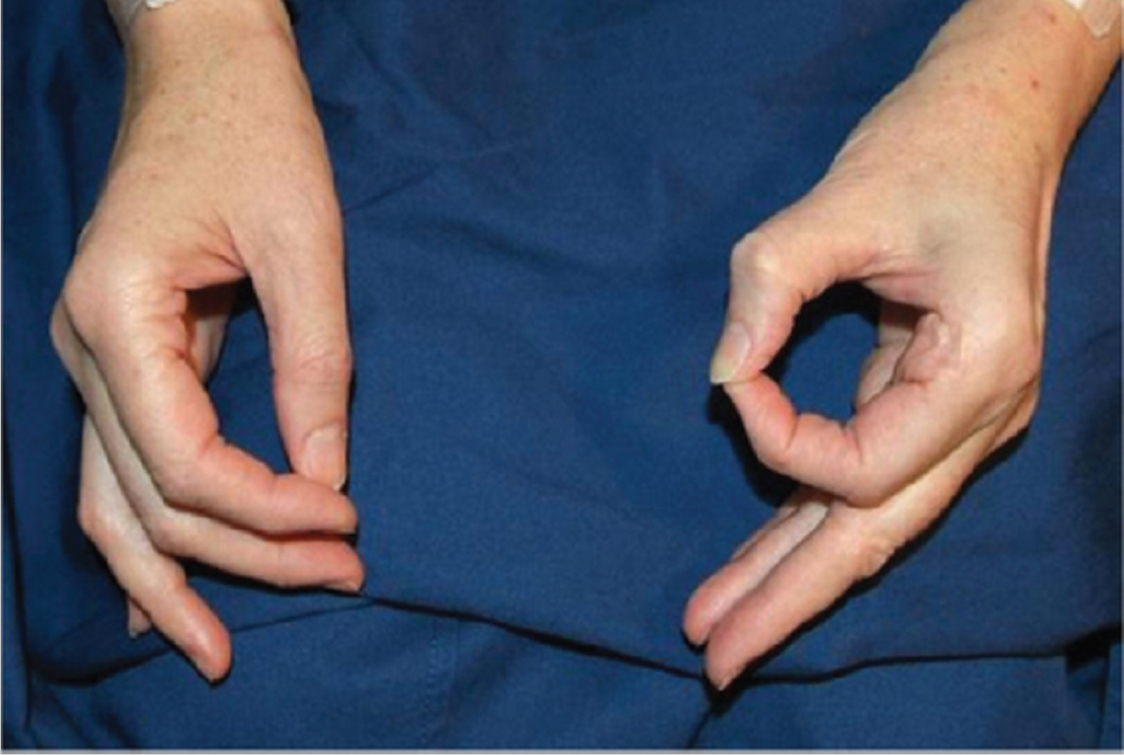
Findings consistent with incomplete median nerve palsy
Intact flexion at proximal interphalangeal joints.
Loss of distal interphalangeal joint flexion of index and long finger and interphalangeal joint of thumb.
Loss of thumb palmar abduction.
Flexion present in right ring and small fingers.
Work-up
History
Age, gender, handedness, and occupation of the patient.
Timing and mechanism of injury
Trauma: Associated injuries, underlying fractures, dislocations, neurovascular insult.
Infection: Nature of infection (bacterial, fungal, other), operative management to date (incision and drainage), antimicrobial medications, local versus systemic signs and symptoms.
Tumor ablation: Tumor pathology, margins, planned radiation and chemotherapy.
Previous injury or surgery to the hand in question.
Manual demands of daily living and overall lifestyle.
Past medical and surgical history.
Social history including smoking status and substance abuse.
Physical examination
Location and type of original injury.
Functional deficit.
Motor function (discern neurologic function based on motor examination findings).
Sensory function.
Vascular status of hand (intact palmar arch).
Pertinent imaging or diagnostic studies
Standard radiography (three views of the hand).
Computed tomography if further detail required regarding bony structures (especially carpal bones).
Consultations
Physical/occupational therapy
If joints are not sufficiently supple, they must be loosened, preferably by hand therapy.
If hand therapy fails, surgical release of the joints may be required before tendon transfer.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


